You might also like
- Comparative Analysis - History of Architecture, China, Japan, KoreaDocument14 pagesComparative Analysis - History of Architecture, China, Japan, KoreaMillenia domingoNo ratings yet
- Outlook Group Written AssignmentDocument34 pagesOutlook Group Written Assignmentashish9dubey-1680% (10)
- Idiopathic Pulmonary Fibrosis: Optimizing The Diagnosis and Multi-Disciplinary Decision MakingDocument4 pagesIdiopathic Pulmonary Fibrosis: Optimizing The Diagnosis and Multi-Disciplinary Decision MakingAnna LiachenkoNo ratings yet
- Idiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistoryDocument11 pagesIdiopathic Pulmonary Fibrosis: Diagnosis, Epidemiology and Natural HistorySuwandi AlghozyNo ratings yet
- Idiopathic Pulmonary Fibrosis: Interstitial Lung DiseaseDocument5 pagesIdiopathic Pulmonary Fibrosis: Interstitial Lung DiseaseAmjaSaudNo ratings yet
- Comptia Linux Xk0 004 Exam Objectives (1 0)Document16 pagesComptia Linux Xk0 004 Exam Objectives (1 0)mueramon100% (1)
- US Dollar Store Consumer BehaviourDocument10 pagesUS Dollar Store Consumer BehaviourTryden Royce D'SouzaNo ratings yet
- List of All ProjectsDocument152 pagesList of All ProjectsMhm ReddyNo ratings yet
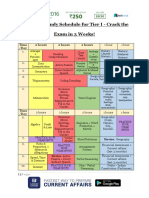
- SSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Document3 pagesSSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Tushita80% (15)
- DR Syed Aqeel Gilani Department of Pulmonology Ayub Teaching Hospital AbbottabadDocument49 pagesDR Syed Aqeel Gilani Department of Pulmonology Ayub Teaching Hospital AbbottabadAnka EremiaNo ratings yet
- Pierre Jeanneret Private ResidencesDocument21 pagesPierre Jeanneret Private ResidencesKritika DhuparNo ratings yet
- User Manual: Shenzhen Biocare Bio-Medical Equipment Co., LTDDocument182 pagesUser Manual: Shenzhen Biocare Bio-Medical Equipment Co., LTDArnaldo AbadNo ratings yet
- Cisco Start CatalogDocument4 pagesCisco Start CatalogqntttNo ratings yet
- Connective Tissue Disease-Associated Interstitial Lung Diseases: Unresolved IssuesDocument9 pagesConnective Tissue Disease-Associated Interstitial Lung Diseases: Unresolved IssuesNuntana ChampaNo ratings yet
- Ali 01Document10 pagesAli 01Juan Fernando Garcia RobledoNo ratings yet
- Comprehensive Review of Current Diagnostic and Treatment Approaches To Interstitial Lung Disease Associated With Rheumatoid ArthritisDocument10 pagesComprehensive Review of Current Diagnostic and Treatment Approaches To Interstitial Lung Disease Associated With Rheumatoid ArthritisskoamdaskondiajosNo ratings yet
- Hata Et Al 2022 Interstitial Lung Abnormalities at CT Subtypes Clinical Significance and Associations With Lung CancerDocument15 pagesHata Et Al 2022 Interstitial Lung Abnormalities at CT Subtypes Clinical Significance and Associations With Lung CancerAndrea PescosolidoNo ratings yet
- Barratt 2018Document21 pagesBarratt 2018Examenes LaboratorioNo ratings yet
- Clinical Significance of Radiological Pleuroparenchymal Fibroelastosis Pattern in Interstitial Lung Disease Patients Registered For Lung Transplantation A Retrospective Cohort StudyDocument11 pagesClinical Significance of Radiological Pleuroparenchymal Fibroelastosis Pattern in Interstitial Lung Disease Patients Registered For Lung Transplantation A Retrospective Cohort StudyFilipe EmanuelNo ratings yet
- Sarcoidosis Review. JAMADocument9 pagesSarcoidosis Review. JAMARafael ReañoNo ratings yet
- 308 895 1 PBDocument4 pages308 895 1 PBNousradine MournoNo ratings yet
- Radiol 2018172688Document10 pagesRadiol 2018172688Nurul Rahmadiani UkfahNo ratings yet
- Richeldi Et Al 2021 Utility of A Molecular Classifier As A Complement To High Resolution Computed Tomography ToDocument10 pagesRicheldi Et Al 2021 Utility of A Molecular Classifier As A Complement To High Resolution Computed Tomography Toحسام الوجيهNo ratings yet
- 2011 in The Clinic - EPOCDocument16 pages2011 in The Clinic - EPOCKarla WevarNo ratings yet
- Pi Is 0954611123001932Document5 pagesPi Is 0954611123001932Angela Fonseca LatinoNo ratings yet
- Review 01-06 PDFDocument6 pagesReview 01-06 PDFEditor IjprtNo ratings yet
- Journal Predictive Factors For Lower Extremity Amputations in Diabetic Foot Infections - Dr. Samuel Jason Rolando Tua TobingDocument6 pagesJournal Predictive Factors For Lower Extremity Amputations in Diabetic Foot Infections - Dr. Samuel Jason Rolando Tua Tobingsamuel3101jasoNo ratings yet
- Risk Factors For Extra-Pulmonary Tuberculosis Compared To Pulmonary TuberculosisDocument6 pagesRisk Factors For Extra-Pulmonary Tuberculosis Compared To Pulmonary TuberculosisLily SmithNo ratings yet
- Ryct 2021200279Document19 pagesRyct 2021200279Andiie ResminNo ratings yet
- Fungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrDocument18 pagesFungalinfections in The Icu: Marya D. Zilberberg,, Andrew F. ShorrGiselle BaiãoNo ratings yet
- Radiologic Manifestations of Pulmonary Tuberculosis in Patients of Intensive Care UnitsDocument6 pagesRadiologic Manifestations of Pulmonary Tuberculosis in Patients of Intensive Care UnitsAnonymous qwH3D0KrpNo ratings yet
- PIIS1076633220302464Document1 pagePIIS1076633220302464India SunshineNo ratings yet
- Impairment Impaimet TBDocument12 pagesImpairment Impaimet TBDoddy KurniawanNo ratings yet
- Atm 04 08 160Document9 pagesAtm 04 08 160manalNo ratings yet
- Machine Learning Automatically Detects Covid-19 Using Chest Cts in A Large Multicenter CohortDocument27 pagesMachine Learning Automatically Detects Covid-19 Using Chest Cts in A Large Multicenter CohortballechaseNo ratings yet
- Post-Tuberculous Chronic Obstructive Pulmonary Disease: Clinical Practice ArticleDocument3 pagesPost-Tuberculous Chronic Obstructive Pulmonary Disease: Clinical Practice ArticleAjeng SekariniNo ratings yet
- Role of Multi-Detector Computed Tomography in Evaluation of Lung AnomaliesDocument16 pagesRole of Multi-Detector Computed Tomography in Evaluation of Lung AnomaliesIJAR JOURNALNo ratings yet
- 1 s2.0 S2772707622001308 MainDocument39 pages1 s2.0 S2772707622001308 MainoscarNo ratings yet
- 100220080112Document8 pages100220080112Nabil MrhiliNo ratings yet
- Infectious Diseases: Chronic Symptoms and Pulmonary Dysfunction in Post-Tuberculosis Brazilian PatientsDocument6 pagesInfectious Diseases: Chronic Symptoms and Pulmonary Dysfunction in Post-Tuberculosis Brazilian PatientsAnonymous Skzf3D2HNo ratings yet
- Ecr2014 C-1725Document8 pagesEcr2014 C-1725HeeroO1No ratings yet
- CT Finding & Dif DX Pulmo AspergiloDocument12 pagesCT Finding & Dif DX Pulmo AspergiloDevi EfrinaNo ratings yet
- Etiologi Efusi PleuraDocument5 pagesEtiologi Efusi Pleuratriska antonyNo ratings yet
- Seminar: EpidemiologyDocument12 pagesSeminar: EpidemiologyPrasasti 19No ratings yet
- The Effect of Diabetes Mellitus On Organ Dysfunction With Sepsis: An Epidemiological StudyDocument6 pagesThe Effect of Diabetes Mellitus On Organ Dysfunction With Sepsis: An Epidemiological StudySintya RadhayantiNo ratings yet
- Pathological Evidence of Pulmonary Thrombotic Phenomena in Severe COVID 19Document5 pagesPathological Evidence of Pulmonary Thrombotic Phenomena in Severe COVID 19Victor AugustoNo ratings yet
- Chronic Rhinosinusitis-An Update On Epidemiology, Pathogenesis and ManagementDocument5 pagesChronic Rhinosinusitis-An Update On Epidemiology, Pathogenesis and ManagementNaufal NrwNo ratings yet
- SaudiJKidneyDisTranspl302470-5143025 141710Document8 pagesSaudiJKidneyDisTranspl302470-5143025 141710AmatystNo ratings yet
- Interstitial Lung Disease After Pleurodesis For Malignant Pleural EffusionDocument7 pagesInterstitial Lung Disease After Pleurodesis For Malignant Pleural EffusionMomoraNo ratings yet
- Concise Clinical Review: Chronic Bronchitis and Chronic Obstructive Pulmonary DiseaseDocument10 pagesConcise Clinical Review: Chronic Bronchitis and Chronic Obstructive Pulmonary DiseaseMuhammad FakhruriNo ratings yet
- Thesis TB and ChestDocument5 pagesThesis TB and Chestirugqgajd100% (1)
- Chronic Rhinosinusitis-An Update On Epidemiology, Pathogenesis and ManagementDocument6 pagesChronic Rhinosinusitis-An Update On Epidemiology, Pathogenesis and ManagementNaufal NrwNo ratings yet
- Patient Handbook BrochureDocument8 pagesPatient Handbook BrochureDr-Yasir Mahmood SyedNo ratings yet
- MainDocument8 pagesMainAbrsham AyeleNo ratings yet
- Rev A - Lung CancerDocument7 pagesRev A - Lung Cancermuhammad irsyad khresna ajiNo ratings yet
- Jact 12 I 2 P 142Document3 pagesJact 12 I 2 P 142Rosdiana Elizabeth Siburian0% (1)
- Chest Radiographic Manifestations of Scrub Typhus - PMCDocument9 pagesChest Radiographic Manifestations of Scrub Typhus - PMCSurachai PraimaiNo ratings yet
- Sjogren ILD1Document12 pagesSjogren ILD1Dra Daphne Rivero GallegosNo ratings yet
- FPI Progn TratDocument13 pagesFPI Progn TratTurcu AndreeaNo ratings yet
- 2018 Article 50Document10 pages2018 Article 50miss betawiNo ratings yet
- Necrotizing Pneumonia in Cancer Patients A.8Document4 pagesNecrotizing Pneumonia in Cancer Patients A.8Manisha UppalNo ratings yet
- Iaet04i4p269 PDFDocument13 pagesIaet04i4p269 PDFjeevan georgeNo ratings yet
- CTS MHDDocument8 pagesCTS MHDTheodoreNo ratings yet
- Improving Risk Stratification of Rheumatoid Arthritis Patients For Intestinal Lung DiseasesDocument11 pagesImproving Risk Stratification of Rheumatoid Arthritis Patients For Intestinal Lung DiseasesdopiorototoNo ratings yet
- Do Inhaled Corticosteroids Protect Against Lung Cancer in Patients With COPD A Systematic ReviewDocument10 pagesDo Inhaled Corticosteroids Protect Against Lung Cancer in Patients With COPD A Systematic ReviewRicovially DavyaNo ratings yet
- CT Scan Findings of Probable Usual Interstitial Pneumonitis Have A High Predictive Value For Histologic Usual Interstitial PneumonitisDocument11 pagesCT Scan Findings of Probable Usual Interstitial Pneumonitis Have A High Predictive Value For Histologic Usual Interstitial PneumonitisMirna Candra DewiNo ratings yet
- Acute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.DDocument12 pagesAcute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.Dkerm6991No ratings yet
- 699-Article Text-1085-1-10-20181101Document6 pages699-Article Text-1085-1-10-20181101Shahid HussainNo ratings yet
- The Papanicolaou Society of Cytopathology System for Reporting Respiratory Cytology: Definitions, Criteria, Explanatory Notes, and Recommendations for Ancillary TestingFrom EverandThe Papanicolaou Society of Cytopathology System for Reporting Respiratory Cytology: Definitions, Criteria, Explanatory Notes, and Recommendations for Ancillary TestingNo ratings yet
- Time Series and Trend Analysis: Presented byDocument11 pagesTime Series and Trend Analysis: Presented byRishabh RajNo ratings yet
- 6to Present Continuous AllDocument1 page6to Present Continuous AllEliana VogtNo ratings yet
- Unit 1 Hello There!: PAG E Lesson Vocabulary Grammar Listening Track: UNIT 1Document10 pagesUnit 1 Hello There!: PAG E Lesson Vocabulary Grammar Listening Track: UNIT 1Analia SanlongNo ratings yet
- FlySmart+ Administrator Course (Windows) - XG04 - 27032024Document4 pagesFlySmart+ Administrator Course (Windows) - XG04 - 27032024steve yangNo ratings yet
- Walt Disney BiographyDocument8 pagesWalt Disney BiographyIsaacRodríguezNo ratings yet
- ICICI - Manufacture in India Fund - Investor One PagerDocument4 pagesICICI - Manufacture in India Fund - Investor One PagerInimitable IdeasNo ratings yet
- Nanthony@uno - Edu: Materials To Bring To The WorkshopDocument2 pagesNanthony@uno - Edu: Materials To Bring To The Workshopenokaconsbio10No ratings yet
- Comp2-Cause-Effect EssayDocument4 pagesComp2-Cause-Effect Essayapi-316060728No ratings yet
- From St. Francis To Dante-Translations From The Chronicle of The Franciscan Salimbene, 1221-1288Document489 pagesFrom St. Francis To Dante-Translations From The Chronicle of The Franciscan Salimbene, 1221-1288Jake SalNo ratings yet
- Petitioner RespondentDocument8 pagesPetitioner RespondentEmNo ratings yet
- Gehman Mennonite Church: Let's Walk With Jesus Personally, Locally, and GloballyDocument1 pageGehman Mennonite Church: Let's Walk With Jesus Personally, Locally, and GloballyGehman Mennonite ChurchNo ratings yet
- Using Density To Determine The Sugar Content in Commercial BeveragesDocument12 pagesUsing Density To Determine The Sugar Content in Commercial BeveragesMax DornelesNo ratings yet
- Levy - Chapter 4Document48 pagesLevy - Chapter 4ANUPAMA RAMACHANDRANNo ratings yet
- Writing Task 2 - Discussion - Opinion EssayDocument7 pagesWriting Task 2 - Discussion - Opinion EssayTonNo ratings yet
- FRC Team 2637, Phatnom Catz, Techbinder 2023 - 2024 CrescendoDocument17 pagesFRC Team 2637, Phatnom Catz, Techbinder 2023 - 2024 CrescendoShrey Agarwal (Drago Gaming)No ratings yet
- Antacyd PDFDocument5 pagesAntacyd PDFIra YunrarzNo ratings yet
- 2011 Issue 3 IPPTA Articel 01Document5 pages2011 Issue 3 IPPTA Articel 01rahulNo ratings yet
- Short VowelDocument3 pagesShort VowelNidzar ZulfriansyahNo ratings yet
- List of Affilited CollegesDocument28 pagesList of Affilited Collegesuzma nisarNo ratings yet
- Intelligent Platform Management Interface Firmware, Upgrade: Operational InstructionDocument23 pagesIntelligent Platform Management Interface Firmware, Upgrade: Operational InstructionLayth WaellNo ratings yet
- Latihan Soal Dan Evaluasi Materi ComplimentDocument6 pagesLatihan Soal Dan Evaluasi Materi ComplimentAvildaAfrinAmmaraNo ratings yet