You might also like
- Discovery NMCT 670 Pro Data SheetDocument16 pagesDiscovery NMCT 670 Pro Data SheetIndarto Julitriarso100% (1)
- Veradius Neo Specs 452296284281 - LRDocument24 pagesVeradius Neo Specs 452296284281 - LRahmed_galal_waly1056No ratings yet
- Infinix 8000Document7 pagesInfinix 8000Khan Kaka100% (1)
- GuideDocument52 pagesGuidemihaelklajner100% (1)
- SP 17M 14 - Preview PDFDocument16 pagesSP 17M 14 - Preview PDFRj KapunanNo ratings yet
- Arbiter Case StudiesDocument110 pagesArbiter Case StudiesChiranjeevi Ram100% (1)
- Catalog MMR Terbaru PDFDocument107 pagesCatalog MMR Terbaru PDFFajar DeniansyahNo ratings yet
- Ecografo Ecofast PhilipsDocument12 pagesEcografo Ecofast PhilipsanayencyramosNo ratings yet
- Toshiba Infinix DP I BrochureDocument8 pagesToshiba Infinix DP I BrochureAhmad AliNo ratings yet
- Toshiba XarioDocument9 pagesToshiba XariowaqasNo ratings yet
- Toshiba Infinix VF I SP BrochureDocument8 pagesToshiba Infinix VF I SP BrochureAhmad Ali100% (1)
- Products Model Company PDFDocument52 pagesProducts Model Company PDFMadhavesh KulkarniNo ratings yet
- Toshiba Infinix CF I BP BrochureDocument8 pagesToshiba Infinix CF I BP BrochureAhmad AliNo ratings yet
- Coil Data Sheet - Dstream WholeBodyDocument2 pagesCoil Data Sheet - Dstream WholeBodylammouchi mariamNo ratings yet
- Brochure - InnoSight GeneralDocument12 pagesBrochure - InnoSight GeneralNurhidayah AyuNo ratings yet
- Multix Select DR: First Time. First ChoiceDocument14 pagesMultix Select DR: First Time. First ChoiceMamdouh AwadNo ratings yet
- Multix Select DR - Data SheetDocument14 pagesMultix Select DR - Data Sheethugo david maldonadoNo ratings yet
- Toshiba Infinix VC I BrochureDocument8 pagesToshiba Infinix VC I BrochureAhmad AliNo ratings yet
- Toshiba Infinix CF I SP BrochureDocument8 pagesToshiba Infinix CF I SP BrochureAhmad AliNo ratings yet
- Tradition With A Future: Solutions For Operative HysterosDocument16 pagesTradition With A Future: Solutions For Operative HysterosMarcus MenezesNo ratings yet
- Comparison of CT Scan Imaging SystemsDocument26 pagesComparison of CT Scan Imaging SystemsUmmi AbubakarNo ratings yet
- Philips BV Pulsera Specs PDFDocument20 pagesPhilips BV Pulsera Specs PDFjose ivan carvajal cortizosNo ratings yet
- Infinix VF I BPDocument8 pagesInfinix VF I BPadalberto VelasNo ratings yet
- Philips Brilliance CT ScannerDocument12 pagesPhilips Brilliance CT ScannerAliali MohamedNo ratings yet
- Mri Hardware Latest TrendDocument30 pagesMri Hardware Latest TrendTechnical SupportNo ratings yet
- Tradition With A Future: Solutions For Operative HysterosDocument16 pagesTradition With A Future: Solutions For Operative Hysterosأحمد قائدNo ratings yet
- Coil Data Sheet - Dstream Flex LDocument2 pagesCoil Data Sheet - Dstream Flex Llammouchi mariamNo ratings yet
- Philips DigitalDiagnost C90 Rel1.1 Specifications Spread Pages (NOV2020)Document27 pagesPhilips DigitalDiagnost C90 Rel1.1 Specifications Spread Pages (NOV2020)kokono8018No ratings yet
- 1025290ra-Isi-Brochure-Single-Site-Digital-Low-Res-394110 BlancDocument10 pages1025290ra-Isi-Brochure-Single-Site-Digital-Low-Res-394110 Blancbarbie11 keira11No ratings yet
- 2-1 박종설.rev1 PDFDocument77 pages2-1 박종설.rev1 PDFNam LeNo ratings yet
- Ficha TEcnica Vivid IQDocument17 pagesFicha TEcnica Vivid IQVanessaNo ratings yet
- Spyglass Detail BrochureDocument12 pagesSpyglass Detail Brochuremaria dolores ramirez roseteNo ratings yet
- New and Featured ProductsDocument16 pagesNew and Featured ProductsHareeshkumar JayakumarNo ratings yet
- Rigid Endoscope User ManualDocument2 pagesRigid Endoscope User Manualأحمد العريقيNo ratings yet
- DC 40 Brochure - En.esDocument8 pagesDC 40 Brochure - En.esMoi KoNo ratings yet
- BodyTom - 12pg1 NL4000 122rev01Document12 pagesBodyTom - 12pg1 NL4000 122rev01KAMENA ObrasNo ratings yet
- ACIST Kodama IVUS Catheter Brochure ENGDocument2 pagesACIST Kodama IVUS Catheter Brochure ENGJia Hui Joana100% (1)
- Toshiba Nemio XGDocument4 pagesToshiba Nemio XGMarco AntonioNo ratings yet
- Asteion Super4Document17 pagesAsteion Super4Godfrey EarnestNo ratings yet
- 2.1 Data Sheet Cios AlphaDocument20 pages2.1 Data Sheet Cios AlphaSóc MâyNo ratings yet
- Vivid Iq 4D Datasheet v9Document17 pagesVivid Iq 4D Datasheet v9Luis Macías BorgesNo ratings yet
- Panorama - Casteellini X Pan85Document12 pagesPanorama - Casteellini X Pan85tito goodNo ratings yet
- Designed For: High Resolution ImagingDocument2 pagesDesigned For: High Resolution ImagingfilibusterosNo ratings yet
- Hitachi - Product GuideDocument10 pagesHitachi - Product Guidezoheb baigNo ratings yet
- Catalog-XC-60-ENG 1.0 - LowDocument8 pagesCatalog-XC-60-ENG 1.0 - LowgaspertrekNo ratings yet
- Philips Affiniti CVXDocument12 pagesPhilips Affiniti CVXkrnl386No ratings yet
- Mindray Resona I9 Ultrasound BrochureDocument4 pagesMindray Resona I9 Ultrasound BrochureHevie MichaelNo ratings yet
- Mindray Resona I9 Brochure Rev B - CR46819Document4 pagesMindray Resona I9 Brochure Rev B - CR46819Walid MohamedNo ratings yet
- Brochure OPTOVUE IScan80Document6 pagesBrochure OPTOVUE IScan80alvinwysNo ratings yet
- OEC Elite II Brochure Arco en C - TouchDocument5 pagesOEC Elite II Brochure Arco en C - TouchAlexander RamirezNo ratings yet
- DP-50 Expert: Ultrasound SystemDocument4 pagesDP-50 Expert: Ultrasound SystembenjaNo ratings yet
- Polestar BrousureDocument20 pagesPolestar BrousureB MNo ratings yet
- Mindray M7 MSK BrochureDocument2 pagesMindray M7 MSK BrochurewanziNo ratings yet
- Palm Vein TechnologyDocument26 pagesPalm Vein TechnologyRakshitha RinkuNo ratings yet
- Opmi Pentero 800Document14 pagesOpmi Pentero 800J JNo ratings yet
- D-Sonosite PX Product BrochureDocument8 pagesD-Sonosite PX Product BrochureArmHSMNo ratings yet
- FS42 p41 ApplTip Quick and Easy Whole Body Scanning With IngeniaDocument4 pagesFS42 p41 ApplTip Quick and Easy Whole Body Scanning With IngeniaJose luis EspinosaNo ratings yet
- Operation Theatre PDFDocument15 pagesOperation Theatre PDFAiswarya AishuuNo ratings yet
- Spesifikasi Brivo XR575Document6 pagesSpesifikasi Brivo XR575ademas podNo ratings yet
- Veradius Neo Product Overview 452296286131 - LRDocument4 pagesVeradius Neo Product Overview 452296286131 - LRahmed_galal_waly1056No ratings yet
- Cardiac Surgical Operative AtlasFrom EverandCardiac Surgical Operative AtlasThorsten WahlersNo ratings yet
- Python - Pandas - Beginner To IntermediateDocument115 pagesPython - Pandas - Beginner To IntermediateName SurnameNo ratings yet
- Deocument - 769full Download Book Nanostructured Carbon Nitrides For Sustainable Energy and Environmental Applications PDFDocument41 pagesDeocument - 769full Download Book Nanostructured Carbon Nitrides For Sustainable Energy and Environmental Applications PDFjohn.greenlee770100% (17)
- Relationship of Nifty-50 With Reliance Infrastructure LTDDocument3 pagesRelationship of Nifty-50 With Reliance Infrastructure LTDPrabhaNo ratings yet
- Test Bank For Elementary Statistics Picturing The World 5 e 5th Edition 0321891872Document11 pagesTest Bank For Elementary Statistics Picturing The World 5 e 5th Edition 0321891872utopiapermix3rNo ratings yet
- AIIMS (MBBS) Solved Question Paper 2010Document34 pagesAIIMS (MBBS) Solved Question Paper 2010cbsestudymaterialsNo ratings yet
- True IronDocument16 pagesTrue IronTecladista ProhibidoNo ratings yet
- Micro SprinklerDocument32 pagesMicro Sprinklerprinceej100% (2)
- Chapter 4 Capacitance PDFDocument12 pagesChapter 4 Capacitance PDFRessyl Mae PantiloNo ratings yet
- Unit 2 Basic Test PDFDocument2 pagesUnit 2 Basic Test PDFAnna SolomennayaNo ratings yet
- 6 Thinking Hats Lesson PlanDocument9 pages6 Thinking Hats Lesson Planapi-409777377No ratings yet
- ZOO 103 Lecture 09 19 ProteinsDocument12 pagesZOO 103 Lecture 09 19 ProteinsKaelyn MontefalconNo ratings yet
- Ásta Categorical InjusticeDocument15 pagesÁsta Categorical InjusticefantasmaNo ratings yet
- Focus2 2E Unit Test Dictation Listening Reading Unit2 GroupADocument2 pagesFocus2 2E Unit Test Dictation Listening Reading Unit2 GroupAКирилл ЗаболоцкийNo ratings yet
- Make Comparison Between Learning Styles of Dunn & Dunn and Kolb Pmi ModelDocument2 pagesMake Comparison Between Learning Styles of Dunn & Dunn and Kolb Pmi ModelSalsabila AinaaNo ratings yet
- IBR IMBUS Datasheet No LogoDocument12 pagesIBR IMBUS Datasheet No Logoenamicul50No ratings yet
- ZOS 1.12 JES2 New FunctionsDocument53 pagesZOS 1.12 JES2 New FunctionsPatrícia RosaNo ratings yet
- Career Resarch Part 2Document4 pagesCareer Resarch Part 2api-478801132No ratings yet
- RopcoverletterDocument1 pageRopcoverletterapi-315542337No ratings yet
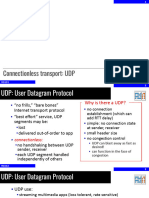
- Connectionless Transport: UDPDocument13 pagesConnectionless Transport: UDPwl.01110111No ratings yet
- LV RV FailureDocument118 pagesLV RV FailureMirza Thaariq HapsitoNo ratings yet
- Five Paragraph OrderDocument8 pagesFive Paragraph OrderBMikeNo ratings yet
- Hiba Kódok Service - TrainingDocument30 pagesHiba Kódok Service - TrainingMiller Andres ArocaNo ratings yet
- "A Generation of Leadership and Excellence" Curriculum VitaeDocument3 pages"A Generation of Leadership and Excellence" Curriculum Vitaebabs23No ratings yet
- Prodelin 1.8m 1184 Assembly Manual PDFDocument24 pagesProdelin 1.8m 1184 Assembly Manual PDFMario SegoviaNo ratings yet
- My Salvation Bewitched and Bewildered 14 - Alanea AlderDocument198 pagesMy Salvation Bewitched and Bewildered 14 - Alanea Aldercoutinholivdalb50% (2)
- Operation Management AssignmentDocument8 pagesOperation Management AssignmentSineshaw AlemuNo ratings yet
- Trend Micro Solution Poster PDFDocument1 pageTrend Micro Solution Poster PDFVăn HảiNo ratings yet
- Blue Ocean BrainDocument2 pagesBlue Ocean BrainJeffrey LodenNo ratings yet