You might also like
- PADI Rescue Diver - Blank Knowledge ReviewDocument13 pagesPADI Rescue Diver - Blank Knowledge ReviewAj Quek67% (3)
- DownloadDocument9 pagesDownloadRhuan AlexandreNo ratings yet
- Cancer Cytopathology - 2020 - Velleuer - Diagnostic Accuracy of Brush Biopsy Based Cytology For The Early Detection of OralDocument11 pagesCancer Cytopathology - 2020 - Velleuer - Diagnostic Accuracy of Brush Biopsy Based Cytology For The Early Detection of Oralopy dasNo ratings yet
- Int Endodontic J - 2021 - Tib Rcio MachadoDocument24 pagesInt Endodontic J - 2021 - Tib Rcio Machadoisabel sotoNo ratings yet
- Metastasis Tumor Ganas Ke Rongga MulutDocument6 pagesMetastasis Tumor Ganas Ke Rongga MulutToothless bdgNo ratings yet
- Articulo 4Document12 pagesArticulo 4Karen CaizaNo ratings yet
- Oral Squamous Cell Carcinoma of Tongue: Histological Risk Assessment. A Pilot StudyDocument7 pagesOral Squamous Cell Carcinoma of Tongue: Histological Risk Assessment. A Pilot StudySaifuddin HaswareNo ratings yet
- Oral Cancer Research PaperDocument4 pagesOral Cancer Research Paperqwmojqund100% (1)
- 10.1007@s00405 020 06036 1Document10 pages10.1007@s00405 020 06036 1yusra ghayoorNo ratings yet
- Medoral 25 E106Document11 pagesMedoral 25 E106Piercy EvaNo ratings yet
- The Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFDocument7 pagesThe Laryngoscope - 2018 - Farhood - Does Anatomic Subsite Influence Oral Cavity Cancer Mortality A SEER Database Analysis PDFJorge JaraNo ratings yet
- Risk Factors of Oral Cancer-A Hospital Based Case Control StudyDocument6 pagesRisk Factors of Oral Cancer-A Hospital Based Case Control StudyDevica DR PutriNo ratings yet
- Artigo 1 ParacococcidiodomicoseDocument9 pagesArtigo 1 Paracococcidiodomicoseandre.jaccoud2No ratings yet
- Pjms 29 1112Document4 pagesPjms 29 1112Diana IancuNo ratings yet
- Biology 12 00239 v2Document18 pagesBiology 12 00239 v2walidNo ratings yet
- 1360 FullDocument5 pages1360 FullLisa Pramitha SNo ratings yet
- Chromosomal Instability, DNA Index, Dysplasia, and SubsiteDocument10 pagesChromosomal Instability, DNA Index, Dysplasia, and SubsiteManar AliNo ratings yet
- Hiv 1 PDFDocument13 pagesHiv 1 PDFmaridaNo ratings yet
- Hed 44 1481Document11 pagesHed 44 1481dayllyn iglesiasNo ratings yet
- Lingen Et Al-2011-Oral DiseasesDocument16 pagesLingen Et Al-2011-Oral DiseasesSAMUEL ESCARESNo ratings yet
- Iej 13 438Document8 pagesIej 13 438raphaNo ratings yet
- Tutorial 2 (New)Document26 pagesTutorial 2 (New)Bilal TahirNo ratings yet
- Articulo 4Document11 pagesArticulo 4Alan SublimeNo ratings yet
- Introduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"Document11 pagesIntroduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"jesus ulises estrada cantuNo ratings yet
- Nasopalatine Duct Cyst Restro StudyDocument8 pagesNasopalatine Duct Cyst Restro StudyTiara Oktavia SaputriNo ratings yet
- Malignant Transformation of Oral Submucous Fibrosis in Taiwan: A Nationwide Population-Based Retrospective Cohort StudyDocument19 pagesMalignant Transformation of Oral Submucous Fibrosis in Taiwan: A Nationwide Population-Based Retrospective Cohort StudyDIVYABOSENo ratings yet
- Student Grant Application Form (PP) - 03 (3) UpdateDocument20 pagesStudent Grant Application Form (PP) - 03 (3) UpdateYousuf SawdagorNo ratings yet
- Global PrevalenceDocument11 pagesGlobal PrevalenceAndres Perez HettingaNo ratings yet
- A Living Biobank of Breast Cancer OrganoidsDocument25 pagesA Living Biobank of Breast Cancer Organoidsfernando dominguezNo ratings yet
- Jof 06 00216 v2Document18 pagesJof 06 00216 v2Grace Yuni Soesanti MhNo ratings yet
- Qualifications For Retinitis Pigmentosa and Leber Congenital Amaurosis Patients For Adeno Associated Viral Gene Replacement Therapy Clinical TrialsDocument10 pagesQualifications For Retinitis Pigmentosa and Leber Congenital Amaurosis Patients For Adeno Associated Viral Gene Replacement Therapy Clinical TrialsAthenaeum Scientific PublishersNo ratings yet
- Cancers 16 01668Document13 pagesCancers 16 01668crochetgawaNo ratings yet
- MastitisDocument5 pagesMastitisAnonymous Kv0sHqFNo ratings yet
- Literature Review PneumoniaDocument4 pagesLiterature Review Pneumoniaafmzahfnjwhaat100% (1)
- Mehanna 2012Document10 pagesMehanna 2012Najib Al FatinNo ratings yet
- Autofluorescence 1Document18 pagesAutofluorescence 1Agache AnamariaNo ratings yet
- HPV and Cervical Cancer Research PaperDocument8 pagesHPV and Cervical Cancer Research Paperafmcuafnh100% (1)
- Int Endodontic J - 2022 - Jakovljevic - Single Nucleotide Polymorphisms As A Predisposing Factor For The Development ofDocument14 pagesInt Endodontic J - 2022 - Jakovljevic - Single Nucleotide Polymorphisms As A Predisposing Factor For The Development ofAKSNo ratings yet
- Onanuga Et Al., Afr., J. Infect. Dis. (2021) 15 (1) : 24-33: Article HistoryDocument10 pagesOnanuga Et Al., Afr., J. Infect. Dis. (2021) 15 (1) : 24-33: Article HistoryTunde OdetoyinNo ratings yet
- Medoralv16 I4 p473Document5 pagesMedoralv16 I4 p473AbhinavNo ratings yet
- Riginal Research: Journal of Advanced Medical and Dental Sciences ResearchDocument3 pagesRiginal Research: Journal of Advanced Medical and Dental Sciences Researchshivam sethiNo ratings yet
- JCDP 21 651Document6 pagesJCDP 21 651Diego GambinNo ratings yet
- Lesões Malignas - Med OralDocument8 pagesLesões Malignas - Med OralCaio GonçalvesNo ratings yet
- MelanomaDocument6 pagesMelanomaagung permanaNo ratings yet
- Survival-Related Epithelial-Mesenchymal Transition Proteins inDocument11 pagesSurvival-Related Epithelial-Mesenchymal Transition Proteins inWeslay Rodrigues da SilvaNo ratings yet
- Biomedicines 12 00703 v2Document19 pagesBiomedicines 12 00703 v2jamel-shamsNo ratings yet
- Advanced Diagnostic Aids in Oral PathologyDocument7 pagesAdvanced Diagnostic Aids in Oral PathologyIJAR JOURNALNo ratings yet
- Omics Editorial 2021Document7 pagesOmics Editorial 2021UMT JournalsNo ratings yet
- W de WenisimoDocument18 pagesW de WenisimoBJ CarminatorNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document8 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Research ParkNo ratings yet
- Better Grade of Tumor Differentiation of Oral Squamous Cell Carcinoma Arising in Background of Oral Submucous FibrosisDocument5 pagesBetter Grade of Tumor Differentiation of Oral Squamous Cell Carcinoma Arising in Background of Oral Submucous FibrosisDIVYABOSENo ratings yet
- Alabi 2019Document8 pagesAlabi 2019Avijit ChaudhuriNo ratings yet
- 10 2334@josnusd 16-0796Document10 pages10 2334@josnusd 16-0796dewi mayaNo ratings yet
- 1 s2.0 S0923753419374125 MainDocument7 pages1 s2.0 S0923753419374125 MainGabriela MonteiroNo ratings yet
- Association of Microbiome With Oral Squamous CellDocument21 pagesAssociation of Microbiome With Oral Squamous CellGhimpu DanielaNo ratings yet
- OM Stafilococo (Clase Observacionales)Document7 pagesOM Stafilococo (Clase Observacionales)Jairo Camilo Guevara FaríasNo ratings yet
- Risk Factors For Medication-Related Osteonecrosis of The Jaws - A Systematic ReviewDocument10 pagesRisk Factors For Medication-Related Osteonecrosis of The Jaws - A Systematic ReviewP.No ratings yet
- 10 1016@j Oraloncology 2019 07 012Document10 pages10 1016@j Oraloncology 2019 07 012Parikesit MuhammadNo ratings yet
- PIIS2212440318300920Document12 pagesPIIS2212440318300920EmiliaAndreeaBalanNo ratings yet
- 2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaDocument7 pages2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaPrasetya AnugrahNo ratings yet
- Practical Lymph Node and Bone Marrow Pathology: Frequently Asked QuestionsFrom EverandPractical Lymph Node and Bone Marrow Pathology: Frequently Asked QuestionsEndi WangNo ratings yet
- Camera CalibrationDocument11 pagesCamera CalibrationFabien MairesseNo ratings yet
- Questions On Function and I T FDocument19 pagesQuestions On Function and I T FNilansh RajputNo ratings yet
- LP Africa (11th Edition)Document406 pagesLP Africa (11th Edition)TucaVieiraNo ratings yet
- ISO 8861 Blower Engine RoomDocument28 pagesISO 8861 Blower Engine Roommohammad choirul huda100% (1)
- Kitchen Window Herb GardenDocument2 pagesKitchen Window Herb GardenNevin SmithNo ratings yet
- Fishery MachinesDocument9 pagesFishery Machinesirshad hussainNo ratings yet
- Bastidas Et Al, 2010Document8 pagesBastidas Et Al, 2010Panji Satria N.No ratings yet
- Chapter 34 - The Influence of Monetary and Fiscal Policy On Aggregate Demand (Compatibility Mode) PDFDocument19 pagesChapter 34 - The Influence of Monetary and Fiscal Policy On Aggregate Demand (Compatibility Mode) PDFthanhvu78No ratings yet
- Industrial Training Sample Report of Last YearDocument42 pagesIndustrial Training Sample Report of Last YearKetan NikamNo ratings yet
- Equipment: MR 51 / MR 51V42 - Handy Power MR 56 / MR 56V42 - Strong PowerDocument4 pagesEquipment: MR 51 / MR 51V42 - Handy Power MR 56 / MR 56V42 - Strong PowerIsmailBelguithNo ratings yet
- 1cobalt Is An Element in Period 4 of The Periodic TableDocument3 pages1cobalt Is An Element in Period 4 of The Periodic TableZigla MooreNo ratings yet
- Embryo AssignmentDocument2 pagesEmbryo AssignmentA.j. MasagcaNo ratings yet
- Dual-Clutch Transmission: Scalable HybridDocument4 pagesDual-Clutch Transmission: Scalable HybridSamadNo ratings yet
- Catalogo EnduroDocument52 pagesCatalogo EnduroCarqtre Carqtre TegNo ratings yet
- Keeling 1960 PDFDocument4 pagesKeeling 1960 PDFErick AmâncioNo ratings yet
- Soal DescriptiveDocument4 pagesSoal DescriptiveLuh SetiawatiNo ratings yet
- Unit Operation QBDocument7 pagesUnit Operation QBsmg26thmayNo ratings yet
- Modified Atmosphere Packaging AssignmentDocument22 pagesModified Atmosphere Packaging AssignmentSanjhai PrakashNo ratings yet
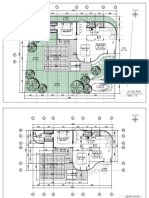
- 2023.01.25 Plan Pecatu Villa - FinishDocument3 pages2023.01.25 Plan Pecatu Villa - FinishTika AgungNo ratings yet
- Scientific Approaches For Impurity Profiling in New Pharmaceutical Substances and Its Products-An OverviewDocument18 pagesScientific Approaches For Impurity Profiling in New Pharmaceutical Substances and Its Products-An OverviewsrichainuluNo ratings yet
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- Bench WorkDocument103 pagesBench Workgetu abrahaNo ratings yet
- FAB-3021117-01-M01-ER-001 - Rev-0 SK-01 & 02Document91 pagesFAB-3021117-01-M01-ER-001 - Rev-0 SK-01 & 02juuzousama1No ratings yet
- Vandex Plug: Rapid-Setting, Crystalline Hydraulic CementDocument2 pagesVandex Plug: Rapid-Setting, Crystalline Hydraulic CementQuerubin EboliNo ratings yet
- Poisson, Poisson-Gamma and Zero-Inflated Regression ModelsDocument43 pagesPoisson, Poisson-Gamma and Zero-Inflated Regression ModelszohrehNo ratings yet
- ACE Inhibitors Vs ARBsDocument3 pagesACE Inhibitors Vs ARBsKo Phyo WaiNo ratings yet
- 7th Chemistry DLP Study Package FinalDocument101 pages7th Chemistry DLP Study Package FinalAdityaNo ratings yet
- 10069-9-V01-Ef00-00039 Fire Alarm SystemDocument49 pages10069-9-V01-Ef00-00039 Fire Alarm Systemahffg nnffNo ratings yet