You might also like
- Nursing 212 Medical - Surgical Nursing 1 PDFDocument178 pagesNursing 212 Medical - Surgical Nursing 1 PDFzarka wahid buxNo ratings yet
- The Effectiveness of Rose Petals and Guava Leaves Extract As A SoapDocument72 pagesThe Effectiveness of Rose Petals and Guava Leaves Extract As A SoapKathy Damaulao80% (5)
- MPH Entrance Examination With AnswersDocument42 pagesMPH Entrance Examination With Answersahmedhaji_sadik94% (87)
- Reyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MDocument50 pagesReyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MGeraldine Marie Salvo100% (1)
- Hang OutDocument92 pagesHang OutMadhu UpadhyayNo ratings yet
- BIOSTAT Post Test Answer KeyDocument13 pagesBIOSTAT Post Test Answer KeyCstive ValenzuelaNo ratings yet
- 2016 OITE Study Guide For ResidentsDocument273 pages2016 OITE Study Guide For Residentschu_chiang_3100% (1)
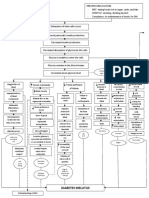
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- Glaucoma Case StudyDocument5 pagesGlaucoma Case StudyEdgel QuidolesNo ratings yet
- Content ON Measurement in Epidemiology Mortality and MorbidityDocument13 pagesContent ON Measurement in Epidemiology Mortality and MorbidityIshika Roy100% (1)
- English For NursesDocument166 pagesEnglish For NursesAlexandrutza IuliaNo ratings yet
- AMA 4351 Statistical EpidemiologyDocument72 pagesAMA 4351 Statistical EpidemiologyRobinson WambuaNo ratings yet
- Microbiology - Bio LibretextDocument782 pagesMicrobiology - Bio LibretextJomsEve Ison100% (2)
- Epidemiology in EmergenciesDocument18 pagesEpidemiology in EmergenciessmartisaacNo ratings yet
- RLE-level-2-packet-week-12-requirement (SANAANI, NUR-FATIMA, M.)Document26 pagesRLE-level-2-packet-week-12-requirement (SANAANI, NUR-FATIMA, M.)Nur SanaaniNo ratings yet
- Strovac Prospect EnglishDocument6 pagesStrovac Prospect EnglishSorin Rusu75% (4)
- General EpidemiologyDocument40 pagesGeneral EpidemiologyrajshreeNo ratings yet
- MPH Entrance Examination With AnswersDocument41 pagesMPH Entrance Examination With Answersmillion assefaNo ratings yet
- Rockson Ohene Asante 2235026 - Epidemiology Assignment by Pratap Kumar Jena SirDocument11 pagesRockson Ohene Asante 2235026 - Epidemiology Assignment by Pratap Kumar Jena SirRockson Ohene AsanteNo ratings yet
- This Module: Covers The Knowledge, Skills and AttitudesDocument13 pagesThis Module: Covers The Knowledge, Skills and AttitudesmeysNo ratings yet
- MPH TestDocument47 pagesMPH Testahmedhaji_sadik50% (2)
- Health and Population IndicatorsDocument68 pagesHealth and Population IndicatorsMarites MaylanonNo ratings yet
- Basic Measures of EpidemiologyDocument51 pagesBasic Measures of EpidemiologyHafiz SabghatullahNo ratings yet
- Copy2-CHAPTER 3Document52 pagesCopy2-CHAPTER 3X And ZNo ratings yet
- Chapter 4-Health Data AnalysisDocument20 pagesChapter 4-Health Data AnalysisNanye AbichNo ratings yet
- Lecture 3. Introduction To EpidemiologyDocument28 pagesLecture 3. Introduction To EpidemiologyHaneen Al-HajjNo ratings yet
- Chapter 101 EpidemiologyDocument44 pagesChapter 101 EpidemiologyYassir OunsaNo ratings yet
- Chintu Zobolo Epidemeology Assignment 2Document7 pagesChintu Zobolo Epidemeology Assignment 2Chintu ZoboloNo ratings yet
- Risk TranscriptDocument14 pagesRisk TranscriptderieNo ratings yet
- CHN Notes For MidtermsDocument24 pagesCHN Notes For MidtermsReiner Lopez100% (1)
- Risk and Frequency: Incidence and Prevalence: Raj BhopalDocument30 pagesRisk and Frequency: Incidence and Prevalence: Raj BhopalWafaa AdamNo ratings yet
- Measurement of Health N DiseaseDocument9 pagesMeasurement of Health N DiseaseOceanChan QdNo ratings yet
- Community Lec4Document19 pagesCommunity Lec4woow0217No ratings yet
- Chapter II - Measurements Used in Epidemiologyoct.22020Document13 pagesChapter II - Measurements Used in Epidemiologyoct.22020Alphine DalgoNo ratings yet
- Science of Epidemiology-31.8.'16 Modified On 23.10.2016Document7 pagesScience of Epidemiology-31.8.'16 Modified On 23.10.2016Alankrit PatnaikNo ratings yet
- Septiya Agestin Cahyaningrum - Resume of Disease Frequency MeasurementDocument17 pagesSeptiya Agestin Cahyaningrum - Resume of Disease Frequency MeasurementSepty KawaiNo ratings yet
- Incidenceandprevalence GangaRamJDocument5 pagesIncidenceandprevalence GangaRamJArdiansyah Yolanda PutraNo ratings yet
- Epidemiological InterpretationDocument9 pagesEpidemiological InterpretationKrishnaveni MurugeshNo ratings yet
- Module 4 Epidemiology and The Nurse (09182021)Document28 pagesModule 4 Epidemiology and The Nurse (09182021)Ariane-Gay Cristobal DuranNo ratings yet
- EpidemiologyDocument66 pagesEpidemiologyTooba NaeemNo ratings yet
- Unit 7 Application of EpidemiologyDocument33 pagesUnit 7 Application of EpidemiologySamantha Adduru100% (1)
- Lesson 4Document59 pagesLesson 4chiyumbabeatriceNo ratings yet
- Week 4 Midterm Study GuideDocument7 pagesWeek 4 Midterm Study GuideDeanne VerschureNo ratings yet
- Measurements of Morbidity & Mortality JayaDocument48 pagesMeasurements of Morbidity & Mortality JayajayalakshmiNo ratings yet
- EpidemiologyDocument18 pagesEpidemiologyRose Jean C. OtodNo ratings yet
- Abhilasha Mali Lecture EpidemologyDocument59 pagesAbhilasha Mali Lecture EpidemologyVikram Singh RanawatNo ratings yet
- Cumulative Incidence MONITORINGDocument67 pagesCumulative Incidence MONITORINGTony Frank RomeoNo ratings yet
- Biostatistic & Epidemic ManagementDocument4 pagesBiostatistic & Epidemic ManagementSAHIL PAREKHNo ratings yet
- Session 1. Intro and Measures of DiseaseDocument10 pagesSession 1. Intro and Measures of DiseaseKato CalebNo ratings yet
- EpidemologyDocument22 pagesEpidemologyVivek MahaleNo ratings yet
- Biostatistic & Epidemic ManagementDocument4 pagesBiostatistic & Epidemic ManagementSAHIL PAREKHNo ratings yet
- PPH4811-Assignment 01Document16 pagesPPH4811-Assignment 01Ivine Sicelo SibekoNo ratings yet
- L3-Meaurements in EpidemiologyDocument34 pagesL3-Meaurements in Epidemiologynewgamesonly101No ratings yet
- PSM LMRP 2019Document25 pagesPSM LMRP 2019skNo ratings yet
- Count, Rate, Ratio, ProportionDocument51 pagesCount, Rate, Ratio, Proportionprasanna lamaNo ratings yet
- Epidemiological StudiesDocument6 pagesEpidemiological StudiesEditor IJTSRDNo ratings yet
- 1-Introduction To PH EpidemiologyDocument33 pages1-Introduction To PH Epidemiologyrabiashoukat7888No ratings yet
- Epidemiological Approach B.SC 4th YearDocument23 pagesEpidemiological Approach B.SC 4th Yearannu panchalNo ratings yet
- 3-Measures of Disease FrequencyDocument34 pages3-Measures of Disease Frequencykeerthi.chowdary.amaraneniNo ratings yet
- RR or Etc 1Document10 pagesRR or Etc 1Thais KnoppNo ratings yet
- An Introduction To EpidemiologyDocument27 pagesAn Introduction To Epidemiologyጀኔራል አሳምነው ፅጌNo ratings yet
- Epidemiology UnitsDocument22 pagesEpidemiology UnitsHikufe JesayaNo ratings yet
- Public Health IDocument78 pagesPublic Health IHardik ParmarNo ratings yet
- Problem OneDocument11 pagesProblem OnePei Qi LimNo ratings yet
- Oral Epidemiology: Epidemiology. Dr. Mohamed Al-MontaserDocument58 pagesOral Epidemiology: Epidemiology. Dr. Mohamed Al-Montaserغلاها عبدوNo ratings yet
- Introduction To Community Dentistry and Dental Public HealthDocument36 pagesIntroduction To Community Dentistry and Dental Public HealthAnosha RiazNo ratings yet
- Epidemiology Lab ManualDocument34 pagesEpidemiology Lab ManualDominique SmithNo ratings yet
- Infectiom Out 4Document23 pagesInfectiom Out 4Yousef AlalawiNo ratings yet
- EL Husseiny's Essentials of Endocrinology 1247Document152 pagesEL Husseiny's Essentials of Endocrinology 1247حنين عاطفNo ratings yet
- Inflammatory Bowel Disease: Ruchita BhavsarDocument34 pagesInflammatory Bowel Disease: Ruchita BhavsarShinta MayasariNo ratings yet
- Abdominal Exam StepsDocument4 pagesAbdominal Exam StepsRonaldoNo ratings yet
- A History of Britain 1945 Through Brexit Jeremy Black Full ChapterDocument51 pagesA History of Britain 1945 Through Brexit Jeremy Black Full Chapteralice.cousin115100% (18)
- Cone Beam CT Literature ReviewDocument6 pagesCone Beam CT Literature Reviewm1dyhuh1jud2100% (1)
- Buteyko Small Manual PDFDocument27 pagesButeyko Small Manual PDFOmmachineNo ratings yet
- Veterinary Dermatology - 2021 - MuellerDocument20 pagesVeterinary Dermatology - 2021 - MuellerMandycat75No ratings yet
- SOP For ASF NRC On PigDocument16 pagesSOP For ASF NRC On PigPallab BorahNo ratings yet
- Defining Cognitive Reserve and Implications For Cognitive AgingDocument12 pagesDefining Cognitive Reserve and Implications For Cognitive AgingmarleimanNo ratings yet
- Slides Multiple SclerosisDocument26 pagesSlides Multiple SclerosisronaNo ratings yet
- UG 1st 2nd 3rd Yr Syllabus BUMS Unani PDFDocument90 pagesUG 1st 2nd 3rd Yr Syllabus BUMS Unani PDFSameer Sam100% (1)
- Family DiagnosisDocument38 pagesFamily DiagnosisRhaden Troy Cristobal GeraliNo ratings yet
- Cancer Bio Lecture 1Document83 pagesCancer Bio Lecture 1snoori2307No ratings yet
- Central Dogma and Genetic MedicineDocument4 pagesCentral Dogma and Genetic MedicineedricNo ratings yet
- Medicine Ophthalmology Slide14Document4 pagesMedicine Ophthalmology Slide14testNo ratings yet
- Spirometry: How To Do The TestDocument4 pagesSpirometry: How To Do The TestMarc AbellaNo ratings yet
- Sensorium.: NiirDocument6 pagesSensorium.: NiirSundar RajanNo ratings yet
- HY RenalDocument50 pagesHY RenalJeniNo ratings yet
- Malawi College of Health Sciences. Clinical Chemistry Examination. 2HRSDocument3 pagesMalawi College of Health Sciences. Clinical Chemistry Examination. 2HRSjames makula100% (1)
- Dengue Fever: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu City College of NursingDocument5 pagesDengue Fever: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu City College of NursingJayson OlileNo ratings yet
- Neha ShahDocument448 pagesNeha ShahAshima GautamNo ratings yet