You might also like
- Nursing Care Plan-Herniated Nucleus PulposusDocument3 pagesNursing Care Plan-Herniated Nucleus PulposusJasmin Jacob67% (3)
- D-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Name Ref. by Test Asked::: Patientid: Home CollectionDocument4 pagesD-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Name Ref. by Test Asked::: Patientid: Home Collectionfaiyaz432No ratings yet
- Basic Safety TrainingDocument70 pagesBasic Safety TrainingMehryl Amponin-Viernes100% (3)
- NUR 200 Tanner's Model - Noticing Through Reflecting-Updated 2020Document4 pagesNUR 200 Tanner's Model - Noticing Through Reflecting-Updated 2020Oliver NamyaloNo ratings yet
- Total Reflexology: The Reflex Points for Physical, Emotional, and Psychological HealingFrom EverandTotal Reflexology: The Reflex Points for Physical, Emotional, and Psychological HealingRating: 2.5 out of 5 stars2.5/5 (2)
- Emergency Nursing CompleteDocument9 pagesEmergency Nursing CompleteggukNo ratings yet
- Review - August 26Document9 pagesReview - August 26hrry stylesNo ratings yet
- UNIT II in HEALTH9 - Injury Prevention Safety and First Aid Unintentional - STUDENTS LectureDocument7 pagesUNIT II in HEALTH9 - Injury Prevention Safety and First Aid Unintentional - STUDENTS Lectureitsmefuntassy100% (1)
- Basic Life Support - 1-18-21 - 2023Document4 pagesBasic Life Support - 1-18-21 - 2023Kim AmadoNo ratings yet
- Basic Life Support - 1 - 18-21 - 2023Document7 pagesBasic Life Support - 1 - 18-21 - 2023Kim AmadoNo ratings yet
- B20M3L5 - Neck InjuriesDocument4 pagesB20M3L5 - Neck InjuriesBarda GulanNo ratings yet
- Multiple TraumaDocument5 pagesMultiple TraumaChristabel EdithNo ratings yet
- Apley Reading - Management of Major InjuriesDocument16 pagesApley Reading - Management of Major InjuriesPatrick LukitoNo ratings yet
- Intro To First AidDocument3 pagesIntro To First AidKyla SaludoNo ratings yet
- Basic First Aid and BLS Reviewer BatchDocument21 pagesBasic First Aid and BLS Reviewer BatchDana Leen GonzalesNo ratings yet
- Basic First Aid and BLS Reviewer Batch PDFDocument21 pagesBasic First Aid and BLS Reviewer Batch PDFDana Leen GonzalesNo ratings yet
- Basic Life Support Webinar NotesDocument5 pagesBasic Life Support Webinar NotesUreh RicardelNo ratings yet
- First AidDocument3 pagesFirst AideliNo ratings yet
- Peri Operative NursingDocument22 pagesPeri Operative NursingIvyBanez100% (1)
- Emergency NursingDocument56 pagesEmergency NursingNur SanaaniNo ratings yet
- Haad RN QuestionDocument7 pagesHaad RN Questionsabu0099No ratings yet
- 6disaster Nursing SAS Session 6Document6 pages6disaster Nursing SAS Session 6Beverly Mae Castillo JaymeNo ratings yet
- HEALTH 9 HandoutsDocument5 pagesHEALTH 9 HandoutsEfren TuvillaNo ratings yet
- Health AssessmentDocument13 pagesHealth AssessmentImee TolentinoNo ratings yet
- Perioperative Nursing NotesDocument13 pagesPerioperative Nursing NotesJuliana Lourdes V. CañadaNo ratings yet
- Poly-Trauma: by Dr. Elias Ahmed October 2003Document14 pagesPoly-Trauma: by Dr. Elias Ahmed October 2003Sisay FentaNo ratings yet
- Medical Surgical NursingDocument66 pagesMedical Surgical Nursing04eden100% (3)
- NCM 119 - Aug. 19, 2021: Emergency Nursing Principles of Emergency CareDocument2 pagesNCM 119 - Aug. 19, 2021: Emergency Nursing Principles of Emergency CareJarod HembradorNo ratings yet
- 59212615-Emergency-Nursing 2Document35 pages59212615-Emergency-Nursing 2Chernobyle Tolentino BattadNo ratings yet
- Polytrauma: Mafalda Sousa Erasmus Student - Tor Vergata Anesthesiology Rome, June 2022Document11 pagesPolytrauma: Mafalda Sousa Erasmus Student - Tor Vergata Anesthesiology Rome, June 2022Mafalda SousaNo ratings yet
- First Aid Lesson HandoutsDocument3 pagesFirst Aid Lesson HandoutsGuia Camandang100% (1)
- General First Aid RescueDocument234 pagesGeneral First Aid RescueJohn Ray BernalNo ratings yet
- BhhuOSaETLGYbjkmhHyxOQ - 3. Approach To The Sick Patient HandoutDocument5 pagesBhhuOSaETLGYbjkmhHyxOQ - 3. Approach To The Sick Patient HandoutStrahinja ŠkoboNo ratings yet
- Perioperative Nursing Is Made Up of 3 Phases What Are TheyDocument2 pagesPerioperative Nursing Is Made Up of 3 Phases What Are TheyAurhea Lyn PrimeroNo ratings yet
- Thuy Functional DimensionDocument3 pagesThuy Functional DimensionTweetie PieNo ratings yet
- Emergency NursingDocument5 pagesEmergency NursingDerick RanaNo ratings yet
- Perioperative Nursing Version 2Document38 pagesPerioperative Nursing Version 2Justine CagatanNo ratings yet
- Care of An Adult Client With Common MentalDocument17 pagesCare of An Adult Client With Common MentalTrisha Lotivio NavarroNo ratings yet
- Emergency Disaster Nursing: Man-Made NaturalDocument2 pagesEmergency Disaster Nursing: Man-Made NaturalVince Rafael Baltazar NuegaNo ratings yet
- Lesson 2Document3 pagesLesson 2soovkaiiiNo ratings yet
- ERDNDocument128 pagesERDNJohiarra TabigneNo ratings yet
- Health Week 1-3 - 3rd QuarterDocument8 pagesHealth Week 1-3 - 3rd QuarterNoemelyn VecinaNo ratings yet
- What Is First Aid?Document2 pagesWhat Is First Aid?Eleina Bea BernardoNo ratings yet
- Basic Life SupportDocument6 pagesBasic Life SupportErrol Flynn S. GarciaNo ratings yet
- Emergency ManagementDocument69 pagesEmergency Managementgiya nursingNo ratings yet
- LESSON PLAN On First Aid GNMDocument6 pagesLESSON PLAN On First Aid GNMSamiran Kumar Das100% (1)
- Emergency MedicineDocument42 pagesEmergency Medicinedrliza75% (8)
- Nursing Lecture NeurologicalDocument28 pagesNursing Lecture NeurologicalAedge010100% (1)
- High Risk ToddlerDocument9 pagesHigh Risk ToddlerasdfghjklNo ratings yet
- Steps to Follow: The Comprehensive Treatment of Patients with HemiplegiaFrom EverandSteps to Follow: The Comprehensive Treatment of Patients with HemiplegiaRating: 5 out of 5 stars5/5 (1)
- Methods of Animal Experimentation: Volume IFrom EverandMethods of Animal Experimentation: Volume IRating: 1 out of 5 stars1/5 (1)
- The Marvels Beyond Science - Being a Record of Progress Made in the Reduction of Occult Phenomena to a Scientific BasisFrom EverandThe Marvels Beyond Science - Being a Record of Progress Made in the Reduction of Occult Phenomena to a Scientific BasisNo ratings yet
- Chronic Pain Management in General and Hospital PracticeFrom EverandChronic Pain Management in General and Hospital PracticeKoki ShimojiNo ratings yet
- Physiology of Man in SpaceFrom EverandPhysiology of Man in SpaceJ. H. U. BrownNo ratings yet
- Saved by the Siesta: fight tiredness and boost your health by unlocking the science of nappingFrom EverandSaved by the Siesta: fight tiredness and boost your health by unlocking the science of nappingNo ratings yet
- Respi-Hema DisordersDocument10 pagesRespi-Hema DisordersggukNo ratings yet
- Fe & EndoDocument14 pagesFe & EndoggukNo ratings yet
- Fundamentals of NursingDocument11 pagesFundamentals of NursingggukNo ratings yet
- Geriatric NursingDocument3 pagesGeriatric NursingggukNo ratings yet
- Cataract - GlaucomaDocument2 pagesCataract - GlaucomaggukNo ratings yet
- PALMRDocument10 pagesPALMRggukNo ratings yet
- Emergency Nursing CompleteDocument9 pagesEmergency Nursing CompleteggukNo ratings yet
- Cattle Diseases Farmers GuideDocument77 pagesCattle Diseases Farmers GuideDivyajyoti DevaNo ratings yet
- Drug Study Ob WardDocument7 pagesDrug Study Ob WardKc DichosoNo ratings yet
- Adhesive Small Bowel Obstruction: Leslie Kobayashi Trauma Conference 2013Document56 pagesAdhesive Small Bowel Obstruction: Leslie Kobayashi Trauma Conference 2013Ananda RizkiNo ratings yet
- Nejmcp 2108502Document9 pagesNejmcp 2108502Manuel GilNo ratings yet
- By:Dr Herbert Sihite Spog: Divisi Feto Maternal FK Usu /rs HamDocument26 pagesBy:Dr Herbert Sihite Spog: Divisi Feto Maternal FK Usu /rs HamDyn AdrianiNo ratings yet
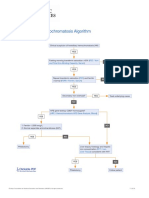
- Hereditary Hemochromatosis AlgorithmDocument1 pageHereditary Hemochromatosis AlgorithmS6b2No ratings yet
- Jadwal Biologi MolekulerDocument1 pageJadwal Biologi Molekulerselfie rijalNo ratings yet
- Vitamin B12 InfographicDocument2 pagesVitamin B12 InfographicIan WynneNo ratings yet
- Screening and Diagnostic Test For Chromosomal DisordersDocument21 pagesScreening and Diagnostic Test For Chromosomal DisordersJohn Van Dave TaturoNo ratings yet
- MeaslesDocument14 pagesMeaslesCHALIE MEQUNo ratings yet
- LicenseSPC PA0002-009-002 16122008220131Document5 pagesLicenseSPC PA0002-009-002 16122008220131abdelaziz_ismail685662No ratings yet
- 4.medicine Side Effect-Plab 2 Nuggets by Ali MunawarDocument3 pages4.medicine Side Effect-Plab 2 Nuggets by Ali MunawarLiviousoeNo ratings yet
- GTS Fact Sheet EnglishDocument2 pagesGTS Fact Sheet EnglishAULIANo ratings yet
- Epilepsy: Presented To Prof - Dr/Shawky Elfiky By/Fatma AdelDocument5 pagesEpilepsy: Presented To Prof - Dr/Shawky Elfiky By/Fatma AdelFatma AdelNo ratings yet
- Differential Diagnosis For The Dermatologist PDFDocument1,352 pagesDifferential Diagnosis For The Dermatologist PDFAndri Sati Siregar80% (5)
- Nodular Calcium & Ivl: 8 JUNE 2023 Bhojraj TiwariDocument57 pagesNodular Calcium & Ivl: 8 JUNE 2023 Bhojraj TiwariNarendra KumarNo ratings yet
- Combined Orals APGODocument52 pagesCombined Orals APGOEmilee Tu0% (1)
- Internal MedicineDocument146 pagesInternal MedicineSh. RamNo ratings yet
- Covid-19 Healthcare Worker Training: Dr. Wangulu Collins (MBCHB, Mmed-Path, MPH) Pathologist - Aar Healthcare (K)Document53 pagesCovid-19 Healthcare Worker Training: Dr. Wangulu Collins (MBCHB, Mmed-Path, MPH) Pathologist - Aar Healthcare (K)odhiambo samwelNo ratings yet
- MCQ in General Surgery For UndergraduatesDocument259 pagesMCQ in General Surgery For UndergraduatesBadri Kobalava100% (5)
- CoopMED Health Insurance Doctor Examination FormDocument2 pagesCoopMED Health Insurance Doctor Examination FormKammieNo ratings yet
- Health Education On DMDocument12 pagesHealth Education On DMAnand Bhawna100% (6)
- Dermatological Toxicities of Bruton's Tyrosine Kinase InhibitorsDocument14 pagesDermatological Toxicities of Bruton's Tyrosine Kinase InhibitorsabdullahNo ratings yet
- Heat EmergenciesDocument3 pagesHeat EmergenciesScott KNo ratings yet
- Getahun Mengistu, MD, MSC, Internist, Neurologist & Specialist in Headache Medicine, Department of Neurology, AAU-MFDocument85 pagesGetahun Mengistu, MD, MSC, Internist, Neurologist & Specialist in Headache Medicine, Department of Neurology, AAU-MFashuNo ratings yet
- Heart Failure Guidelines For India Update 2017Document6 pagesHeart Failure Guidelines For India Update 2017Aditya SutarNo ratings yet
- 27 Ovarian Cystectomy Consent FormDocument3 pages27 Ovarian Cystectomy Consent FormsekyNo ratings yet
- AkiDocument20 pagesAkiEnvhy AmaliaNo ratings yet