You might also like
- Schizophrenia Spectrum and Other Psychotic DisorderDocument7 pagesSchizophrenia Spectrum and Other Psychotic DisorderLorraine0% (1)
- Addiction BrainDocument2 pagesAddiction BrainmelodyfathiNo ratings yet
- 3rd Grade - 3Document19 pages3rd Grade - 3Redgie G. GabaneNo ratings yet
- Understanding The Disease of Addiction: Kathy Bettinardi-Angres, MS, RN, APN, CADC, and Daniel H. Angres, MDDocument7 pagesUnderstanding The Disease of Addiction: Kathy Bettinardi-Angres, MS, RN, APN, CADC, and Daniel H. Angres, MDESTHER OGODONo ratings yet
- Doctor Profile Format Dr. Sarika Trimbak Shinde, MSDocument3 pagesDoctor Profile Format Dr. Sarika Trimbak Shinde, MSSwapnil JaikarNo ratings yet
- Mnemonic SDocument42 pagesMnemonic SWen Jie LauNo ratings yet
- Women's Health & Physical Rehabilitation.Document31 pagesWomen's Health & Physical Rehabilitation.Arham ShamsiNo ratings yet
- Screening, Diagnosis and Early Intervention in Autism Spectrum DisordersDocument5 pagesScreening, Diagnosis and Early Intervention in Autism Spectrum DisordersDaniele PendezaNo ratings yet
- Duty Week 2: Etiologic/Causative Factors: Increased Risk For Death From Other Causes IncludingDocument5 pagesDuty Week 2: Etiologic/Causative Factors: Increased Risk For Death From Other Causes IncludingMeryville JacildoNo ratings yet
- FAMILY NURSING CARE PLAN - Alcohol DrinkingDocument2 pagesFAMILY NURSING CARE PLAN - Alcohol DrinkingJULIANNE BAYHONNo ratings yet
- Substance-Related DisorderDocument2 pagesSubstance-Related DisorderRichelle Delos ReyesNo ratings yet
- AaaaaaaaaaaaaaaaaaaaaaaaaaaDocument4 pagesAaaaaaaaaaaaaaaaaaaaaaaaaaaKatrina AballaNo ratings yet
- Alcohol Drinking FNCPDocument2 pagesAlcohol Drinking FNCPCzar BartolomeNo ratings yet
- Disturbed Thought Processes DescribeDocument2 pagesDisturbed Thought Processes DescribePRINCESS LARA CASILAONo ratings yet
- HALOPERIDOL Drug StudyDocument2 pagesHALOPERIDOL Drug Studyanreilegarde89% (9)
- NCM 114 Care For Older Adults MODULE 4Document5 pagesNCM 114 Care For Older Adults MODULE 4Meryville JacildoNo ratings yet
- Kidney Cancer Principles and Practice by Primo N. Lara, Eric JonaschDocument400 pagesKidney Cancer Principles and Practice by Primo N. Lara, Eric JonaschCoralina100% (2)
- Telephone Directory October-2020-20Document40 pagesTelephone Directory October-2020-20Sameer BakshiNo ratings yet
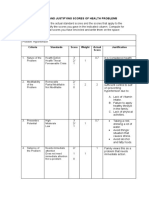
- C.2 Computing and Justifying Score of Health ProblemsDocument3 pagesC.2 Computing and Justifying Score of Health ProblemsHannah Angelu Cabading100% (1)
- Presentation 13 Mental Health Epilepsy and AutismDocument31 pagesPresentation 13 Mental Health Epilepsy and AutismTresor MbuyiNo ratings yet
- AddictionsDocument2 pagesAddictionsEvelin Jazmin Hernández OrtizNo ratings yet
- NCM 105 RLE Case 2Document8 pagesNCM 105 RLE Case 2Maria Charis Anne IndananNo ratings yet
- NSG Care Plan - BipolarDocument17 pagesNSG Care Plan - BipolaraijelethdaldeavilaNo ratings yet
- Vice and Drugs Education Reviewer - 070753Document16 pagesVice and Drugs Education Reviewer - 070753alliahshane.borromeoNo ratings yet
- Learning Objectives: Nstp-Cwts I Module 1 - Drug Education in The PhilippinesDocument13 pagesLearning Objectives: Nstp-Cwts I Module 1 - Drug Education in The PhilippinesALMONIA, GEZZIEL GANIRNo ratings yet
- Module 4Document13 pagesModule 4Cathlyne Mejia NatnatNo ratings yet
- Nursing Care Plan MulletDocument4 pagesNursing Care Plan MulletMARLA PHOEBE KYTE MULLETNo ratings yet
- Abnormal Psychology-Substance Related DisordersDocument2 pagesAbnormal Psychology-Substance Related DisordersMyk AbayaNo ratings yet
- Abnormal Pscych 8-11Document6 pagesAbnormal Pscych 8-11CLAUDINE DOLINONo ratings yet
- DRUGSDocument2 pagesDRUGSchelcieariendeleonNo ratings yet
- 2-Calcium Channel Blockers (Nifedipine) 3 - ImmunosuppressantsDocument1 page2-Calcium Channel Blockers (Nifedipine) 3 - Immunosuppressantsmohamed saadNo ratings yet
- Cannabis and Hallucinogen RelatedDocument22 pagesCannabis and Hallucinogen RelatedEdna Itzel Chavez HernandezNo ratings yet
- Anusha Sharma - Impact of Digital Education On Mental Health of StudentsDocument13 pagesAnusha Sharma - Impact of Digital Education On Mental Health of StudentsAnusha SharmaNo ratings yet
- DexamethasoneDocument1 pageDexamethasoneACOB, Jamil C.No ratings yet
- DRUG STUDY - AnticonvulsantsDocument1 pageDRUG STUDY - AnticonvulsantsZam PamateNo ratings yet
- NSTP2 Module 4 AssignmentDocument2 pagesNSTP2 Module 4 AssignmentmikomikomikNo ratings yet
- Disorders With Increased Risk of Drug AbuseDocument2 pagesDisorders With Increased Risk of Drug AbuselosangelesNo ratings yet
- Assessment Explanation of The Problem Objectives Intervention Rationale EvaluationDocument2 pagesAssessment Explanation of The Problem Objectives Intervention Rationale EvaluationDyanne BautistaNo ratings yet
- Stop Drugs 4 y 5Document1 pageStop Drugs 4 y 5Rosa Marleni Valentin PalominoNo ratings yet
- Problem # 2: Lifestyle (Smoking & Alcohol) Assessment Plan Intervention EvaluationDocument4 pagesProblem # 2: Lifestyle (Smoking & Alcohol) Assessment Plan Intervention EvaluationAnastasya Gishella RorongNo ratings yet
- Drugs of AbuseDocument9 pagesDrugs of AbuseCrisheila Sarah PiedadNo ratings yet
- Community Health Nursing Care PlanDocument4 pagesCommunity Health Nursing Care Plankate russelNo ratings yet
- FNCP TemplateDocument2 pagesFNCP TemplateMary Ann Sambo OgoyNo ratings yet
- Bipolar DisorderDocument2 pagesBipolar DisorderChristel Mariz SantellaNo ratings yet
- Management: Delirium Assessment and Treatment For Older AdultsDocument2 pagesManagement: Delirium Assessment and Treatment For Older Adultsramzan aliNo ratings yet
- Advocacy Brochure - Health (Elisa)Document3 pagesAdvocacy Brochure - Health (Elisa)Elisa Cielo NecesarioNo ratings yet
- Drug Education 1Document41 pagesDrug Education 1REYES JANA ACETINENo ratings yet
- NCP Mugar Icu3 Batch2 GRP3Document2 pagesNCP Mugar Icu3 Batch2 GRP3FRANZI ALYANNA MUGARNo ratings yet
- Substance AbuseDocument5 pagesSubstance Abusejuliene13No ratings yet
- The Effects of White Noise On Agitated BehaviorsDocument8 pagesThe Effects of White Noise On Agitated BehaviorsTestNo ratings yet
- Daat11i2p199 PDFDocument6 pagesDaat11i2p199 PDFAngeline PutriNo ratings yet
- Substance-Related Disorders: Professor DR Sirwan K Ali Department of PsychiatryDocument43 pagesSubstance-Related Disorders: Professor DR Sirwan K Ali Department of PsychiatryAlan AhmadNo ratings yet
- TABLE Prioritization and Ranking of Problems 11Document5 pagesTABLE Prioritization and Ranking of Problems 11Jasmine CorreosNo ratings yet
- Long Term Care ServicesDocument8 pagesLong Term Care ServicesCole GoNo ratings yet
- With RationaleDocument4 pagesWith RationaleKaren mae alvarroNo ratings yet
- Substance - Related DisorderDocument6 pagesSubstance - Related DisorderMitzi BelamideNo ratings yet
- Psych Vignetter VC Group 5Document20 pagesPsych Vignetter VC Group 5ErleNo ratings yet
- Agot Rle Case Study 3Document17 pagesAgot Rle Case Study 3Angel May P AgotNo ratings yet
- Cns Drugs Summary Review Notes FinalDocument12 pagesCns Drugs Summary Review Notes Finalمريم حجيNo ratings yet
- St. Michael's College: Nursing Care Plan FormDocument3 pagesSt. Michael's College: Nursing Care Plan Formacademic purposesNo ratings yet
- 117a MidtermDocument2 pages117a MidtermJonathan MangawiliNo ratings yet
- CDI7 SemisDocument4 pagesCDI7 SemisMa. Teresa FloresNo ratings yet
- ACFrOgDeZ3FQkI84X1GQy8u5a0Nep5UKNESbHpzKyqBBtHk SWLnA4LqdE2PS1Yawhawr1mOLnvLmG2BbNhjmglb Zlow1zL6Bc94qwxJC7yzl-bsOCzFhRsza1piHY pmJJm-vpifzcNjsrsFdpDocument16 pagesACFrOgDeZ3FQkI84X1GQy8u5a0Nep5UKNESbHpzKyqBBtHk SWLnA4LqdE2PS1Yawhawr1mOLnvLmG2BbNhjmglb Zlow1zL6Bc94qwxJC7yzl-bsOCzFhRsza1piHY pmJJm-vpifzcNjsrsFdpKristel Kate Melchor TugadeNo ratings yet
- Drug StudyDocument2 pagesDrug StudyCherry CayabyabNo ratings yet
- JPSP - 2022 - 199Document7 pagesJPSP - 2022 - 199Pes ForNo ratings yet
- The Bipolar Disorder Survival Guide: Step-by-Step Strategies for Living and Thriving with Bipolar DisorderFrom EverandThe Bipolar Disorder Survival Guide: Step-by-Step Strategies for Living and Thriving with Bipolar DisorderNo ratings yet
- Aca Code of EthicsDocument25 pagesAca Code of EthicsRedgie G. GabaneNo ratings yet
- Dissociative DisordersDocument1 pageDissociative DisordersRedgie G. GabaneNo ratings yet
- Somatic DisordersDocument3 pagesSomatic DisordersRedgie G. GabaneNo ratings yet
- Psychological AssessmentDocument2 pagesPsychological AssessmentRedgie G. GabaneNo ratings yet
- Table of Specifications (TOS) - BLEPP 2024Document8 pagesTable of Specifications (TOS) - BLEPP 2024Redgie G. GabaneNo ratings yet
- Trauma and Stressor Related DisordersDocument2 pagesTrauma and Stressor Related DisordersRedgie G. GabaneNo ratings yet
- DEVPSYCH 9 - Physical and Cognitive Development in Middle ChildhoodDocument3 pagesDEVPSYCH 9 - Physical and Cognitive Development in Middle ChildhoodRedgie G. GabaneNo ratings yet
- Thesis Chapter 1 - 2 - 3Document23 pagesThesis Chapter 1 - 2 - 3Redgie G. GabaneNo ratings yet
- NeurotransmittersDocument1 pageNeurotransmittersRedgie G. GabaneNo ratings yet
- Thesis - SurveyDocument9 pagesThesis - SurveyRedgie G. GabaneNo ratings yet
- Ensuring Fair Testing Practices For Test TakerDocument36 pagesEnsuring Fair Testing Practices For Test TakerRedgie G. GabaneNo ratings yet
- DEVPSYCH 7 - Physical and Cognitive Development in Early ChildhoodDocument4 pagesDEVPSYCH 7 - Physical and Cognitive Development in Early ChildhoodRedgie G. GabaneNo ratings yet
- PDYCH AS Drills Top RankDocument15 pagesPDYCH AS Drills Top RankRedgie G. GabaneNo ratings yet
- Comer SummaryDocument50 pagesComer SummaryRedgie G. GabaneNo ratings yet
- DEVPSYCH 6 - Psychosocial Development During The First 3 YearsDocument3 pagesDEVPSYCH 6 - Psychosocial Development During The First 3 YearsRedgie G. GabaneNo ratings yet
- DEVPSYCH 8 - Psychosocial Development in Early ChildhoodDocument3 pagesDEVPSYCH 8 - Psychosocial Development in Early ChildhoodRedgie G. GabaneNo ratings yet
- MBTI StepDocument21 pagesMBTI StepRedgie G. GabaneNo ratings yet
- Tpa CH 3Document60 pagesTpa CH 3Redgie G. GabaneNo ratings yet
- Developmental Psychology Chapter 8 Old AgeDocument7 pagesDevelopmental Psychology Chapter 8 Old AgeRedgie G. GabaneNo ratings yet
- DEVPSYCH 5 - Cognitive Development During The First 3 YearsDocument3 pagesDEVPSYCH 5 - Cognitive Development During The First 3 YearsRedgie G. GabaneNo ratings yet
- Reliability Vs ValidityDocument27 pagesReliability Vs ValidityRedgie G. GabaneNo ratings yet
- A Review of Employees' Well-Being, Psychological Factors and Its Effect On Job Performance LiteratureDocument12 pagesA Review of Employees' Well-Being, Psychological Factors and Its Effect On Job Performance LiteratureRedgie G. GabaneNo ratings yet
- PEC Module 1Document164 pagesPEC Module 1Redgie G. GabaneNo ratings yet
- Known Group MethodDocument11 pagesKnown Group MethodRedgie G. GabaneNo ratings yet
- Procedures For Assessing The Validities of Tests UDocument12 pagesProcedures For Assessing The Validities of Tests URedgie G. GabaneNo ratings yet
- Test DesignDocument28 pagesTest DesignRedgie G. GabaneNo ratings yet
- Psych Quiz-1Document23 pagesPsych Quiz-1Redgie G. GabaneNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFRedgie G. GabaneNo ratings yet
- Psych Assessment-2Document22 pagesPsych Assessment-2Redgie G. GabaneNo ratings yet
- Post-ACLS Megacode Flashcards - QuizletDocument9 pagesPost-ACLS Megacode Flashcards - QuizletMaya LaPradeNo ratings yet
- ETT Vs LMADocument33 pagesETT Vs LMAitaindrianiNo ratings yet
- Marijuana Use and Breastfeeding PDFDocument7 pagesMarijuana Use and Breastfeeding PDFmdbackesNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- L03 - 04 EEG MondayDocument10 pagesL03 - 04 EEG MondayShawn SequeiraNo ratings yet
- Tetralogy of FallotDocument3 pagesTetralogy of FallotKamal FauzeNo ratings yet
- SchistosomiasisDocument3 pagesSchistosomiasisglaire927No ratings yet
- Hyperbaric Oxygen Therapy (Hbot) : Presented by DR Manu Bhaskaran NairDocument55 pagesHyperbaric Oxygen Therapy (Hbot) : Presented by DR Manu Bhaskaran NairMahipal Reddy NimmalaNo ratings yet
- Riscuri DP DuodenopancreatectomieDocument7 pagesRiscuri DP DuodenopancreatectomieAndreea StanescuNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsKirubairajNo ratings yet
- Tumor Traktus UrogenitalDocument23 pagesTumor Traktus UrogenitalganmarifNo ratings yet
- Polymyxin B: Similarities To and Differences From Colistin (Polymyxin E)Document12 pagesPolymyxin B: Similarities To and Differences From Colistin (Polymyxin E)Anggun NurhidayahNo ratings yet
- Morning Shift Report: Emergency RoomDocument11 pagesMorning Shift Report: Emergency RoomIputu Abhi Acarya SaputraNo ratings yet
- Ashwagandha Leaves Medicinal UsesDocument3 pagesAshwagandha Leaves Medicinal UsesSanjay PatilNo ratings yet
- Non-Suppurative Otitis MediaDocument20 pagesNon-Suppurative Otitis MediasaymynamesNo ratings yet
- Mushtaq Ahmad: Running Head: REFLECTIVE LOG 1Document5 pagesMushtaq Ahmad: Running Head: REFLECTIVE LOG 1Shafiq Ur RahmanNo ratings yet
- He - Sample of Informed ConsentDocument2 pagesHe - Sample of Informed ConsentGwen SolanoNo ratings yet
- Haley Hudgin CVT Echo ResumeDocument2 pagesHaley Hudgin CVT Echo Resumeapi-320308843No ratings yet
- Supply Disruption AlertDocument5 pagesSupply Disruption AlertM Teresa LeivaNo ratings yet
- Brompheniramine (Bromax, Lodrane)Document8 pagesBrompheniramine (Bromax, Lodrane)Asniah Hadjiadatu AbdullahNo ratings yet
- Congress Program September 2022 Anglisht 1 1Document17 pagesCongress Program September 2022 Anglisht 1 1ediNo ratings yet
- Dental Hospital in VijayawadaDocument9 pagesDental Hospital in Vijayawadakrishna dentalNo ratings yet
- Micro Lab 11Document3 pagesMicro Lab 11goatsecksNo ratings yet
- Peter Collins Nutrition Support Severe Respiratory Disease 3 Slides PPDocument19 pagesPeter Collins Nutrition Support Severe Respiratory Disease 3 Slides PPKim Nana UlfaNo ratings yet