You might also like
- MVS205 Multi-Variable Sensor: Specification SheetDocument2 pagesMVS205 Multi-Variable Sensor: Specification SheetjoshNo ratings yet
- Babylog-Vn500 With HFODocument10 pagesBabylog-Vn500 With HFOABHINANDAN SHARMANo ratings yet
- Ventilation Servo-I Universal: Data SheetDocument16 pagesVentilation Servo-I Universal: Data SheetridercoderNo ratings yet
- Evita v300 Pi 9067780 enDocument8 pagesEvita v300 Pi 9067780 ensahal backNo ratings yet
- Festo Electovalvulas Guia de SeleccionDocument2 pagesFesto Electovalvulas Guia de SeleccionhomeroNo ratings yet
- WATO EX-65 Pro - Brochure - ENG - 20180627 - SDocument4 pagesWATO EX-65 Pro - Brochure - ENG - 20180627 - SSandra MacarenoNo ratings yet
- Modes-Of-Ventilation LM en A02 02Document56 pagesModes-Of-Ventilation LM en A02 02Leonardo PeñaNo ratings yet
- Dokumen - Tips Abb Powerpoint Transformer Components Because Reliability Is Everything Vacuum OltcDocument29 pagesDokumen - Tips Abb Powerpoint Transformer Components Because Reliability Is Everything Vacuum OltcKiran KarthikNo ratings yet
- FLOW I BROCHU Anesthesia Delivery SystemDocument12 pagesFLOW I BROCHU Anesthesia Delivery SystemஅNo ratings yet
- Modes of Ventilation H L en A02 01a NPDocument55 pagesModes of Ventilation H L en A02 01a NPSayan SenNo ratings yet
- SERVO-Air Presentation Indonesia Rev SlideDocument32 pagesSERVO-Air Presentation Indonesia Rev SlideSamsulNo ratings yet
- Boaray 5000D Ventilator Introduction - V8.1 - EN-1Document19 pagesBoaray 5000D Ventilator Introduction - V8.1 - EN-1Moch YusufNo ratings yet
- Modulair EngDocument5 pagesModulair EngJaned PerwiraNo ratings yet
- Bellavista 1000 Technical - SpecificationsDocument4 pagesBellavista 1000 Technical - SpecificationsTri DemarwanNo ratings yet
- Intensive Care Ventilator MV200: Safety - Reliability - ComfortDocument7 pagesIntensive Care Ventilator MV200: Safety - Reliability - ComfortFathur ArRahmanNo ratings yet
- Briovent VentilatorDocument10 pagesBriovent VentilatorPurchase DepartmentNo ratings yet
- 4WE10 New Series Directional Valves NG10Document9 pages4WE10 New Series Directional Valves NG10Paulo ArrudaNo ratings yet
- 4WE10 New Series Directional Valves NG10Document9 pages4WE10 New Series Directional Valves NG10Paulo ArrudaNo ratings yet
- P10120en2109 Ventilation Info-1Document8 pagesP10120en2109 Ventilation Info-1Salman SaeedNo ratings yet
- Dräger Savina® Sub-Acute Care VentilationDocument6 pagesDräger Savina® Sub-Acute Care VentilationTeguh KurniawanNo ratings yet
- Ventilator: Shenzhen Comen Medical Instruments Co., LTDDocument4 pagesVentilator: Shenzhen Comen Medical Instruments Co., LTDSoporte BiosummaNo ratings yet
- SV300 Ventilator Product BrochureDocument6 pagesSV300 Ventilator Product BrochureabnerkalilNo ratings yet
- Vtus-G enDocument223 pagesVtus-G enJosé Pedro MarcondesNo ratings yet
- Tv-100 Ventilator: Infant - Pediatric - Adult / ICU-TransportDocument4 pagesTv-100 Ventilator: Infant - Pediatric - Adult / ICU-Transportsouad souadNo ratings yet
- Ivalve Ibox Wechsel - 300 S 9010554 enDocument15 pagesIvalve Ibox Wechsel - 300 S 9010554 enecrgvpNo ratings yet
- Applications Guide: Pneumatic VAV Reset Volume ControllersDocument15 pagesApplications Guide: Pneumatic VAV Reset Volume ControllersSean ByrneNo ratings yet
- Pneumatic Valves VUWS/valve Manifold Assembly VTUSDocument142 pagesPneumatic Valves VUWS/valve Manifold Assembly VTUSnyuvaraj603No ratings yet
- Keymc 0153 UsDocument8 pagesKeymc 0153 UsluisNo ratings yet
- Vyr Int 1900003 Bellavista 1000 TechspecsDocument16 pagesVyr Int 1900003 Bellavista 1000 Techspecshüseyin vururNo ratings yet
- Clinical Advancement, Ease of Use, Versatility, - in and Out of The ICUDocument6 pagesClinical Advancement, Ease of Use, Versatility, - in and Out of The ICUmatijahNo ratings yet
- Electric Valve Actuators VA 7450 SeriesDocument7 pagesElectric Valve Actuators VA 7450 SeriescesarintiNo ratings yet
- Adult Breathing Systems For Transport VentilatorsDocument4 pagesAdult Breathing Systems For Transport Ventilatorstaniamr11No ratings yet
- Keymc 0153 UsDocument8 pagesKeymc 0153 UsDaniel BahamondeNo ratings yet
- Introduction To Lyra Icu Ventilator: Axcent Medical GMBHDocument18 pagesIntroduction To Lyra Icu Ventilator: Axcent Medical GMBHRamadhan Febri100% (1)
- H Series Valves-EN PDFDocument12 pagesH Series Valves-EN PDFMauricio GarciaNo ratings yet
- Ab 6739 PDFDocument16 pagesAb 6739 PDFRendy MulyadiNo ratings yet
- VAV Air Terminal UnitsDocument11 pagesVAV Air Terminal Unitsbrian mmec2020No ratings yet
- NV 24 Globe ActuatorDocument12 pagesNV 24 Globe ActuatorRodrigo AlvesNo ratings yet
- Vela Ventilator Series ComparisonDocument16 pagesVela Ventilator Series ComparisonJason BroughallNo ratings yet
- Ventilation Servo-I Universal: Data SheetDocument20 pagesVentilation Servo-I Universal: Data SheetBreno VieiraNo ratings yet
- NFBUP NFXUP S-Sub1 PDFDocument2 pagesNFBUP NFXUP S-Sub1 PDFMihai Butnaru-PaladeNo ratings yet
- GE VS Phlips FDA PDFDocument12 pagesGE VS Phlips FDA PDFee113051No ratings yet
- VDX 2500 Valve DistribuitorDocument5 pagesVDX 2500 Valve DistribuitorMichael ManzanoNo ratings yet
- DocsheetDocument2 pagesDocsheetMarija DenićNo ratings yet
- Flowmeters: Sitrans F VaDocument7 pagesFlowmeters: Sitrans F VachochoroyNo ratings yet
- WATO EX 65 Pro - BrochureDocument4 pagesWATO EX 65 Pro - BrochureMohamed KhaledNo ratings yet
- BA - BV Series Air Hammer Pneumatic Vibrator - B0Document16 pagesBA - BV Series Air Hammer Pneumatic Vibrator - B0Nguyễn Ngọc Phước VươngNo ratings yet
- Accutherm Honeywell Vq400m Series Combination Gas Valve 140130100612Document15 pagesAccutherm Honeywell Vq400m Series Combination Gas Valve 140130100612Wily WayerNo ratings yet
- SMC 56 PA3110 F03 Datasheet PDFDocument37 pagesSMC 56 PA3110 F03 Datasheet PDFDaniela ZavalaNo ratings yet
- FT 1000 - FP 1000 - TG L111eDocument12 pagesFT 1000 - FP 1000 - TG L111eaditya pamungkasNo ratings yet
- Allied Autovent 2000 3000 ManualDocument28 pagesAllied Autovent 2000 3000 ManualwiroarNo ratings yet
- Newport E200 WaveDocument1 pageNewport E200 Wavesamlu71No ratings yet
- SV300 Service Training-Basic V1.0Document82 pagesSV300 Service Training-Basic V1.0WALTER HUGO GOMEZNo ratings yet
- SynoVent E5Document29 pagesSynoVent E5Adi BimBim SetiawanNo ratings yet
- Vyr Int 1900001 Bellavista 1000e TechspecsDocument16 pagesVyr Int 1900001 Bellavista 1000e Techspecshüseyin vururNo ratings yet
- MVHF DBL334eDocument2 pagesMVHF DBL334eGOOGLE DISKNo ratings yet
- Vtug-G en PDFDocument215 pagesVtug-G en PDFrzezniccNo ratings yet
- FT 1000 - FP 1000 - TG L111eDocument12 pagesFT 1000 - FP 1000 - TG L111eoni tofanNo ratings yet
- Versatile Anestheisia MachineDocument2 pagesVersatile Anestheisia MachineaksinuNo ratings yet
- Sentinel DCS System: FeaturesDocument2 pagesSentinel DCS System: FeaturesEnderson Ramos100% (1)
- Class 7 Science MCQSDocument176 pagesClass 7 Science MCQSAnieKhan100% (3)
- Copernicus Natural Science Category 3: Grades 7-8 Practice PaperDocument29 pagesCopernicus Natural Science Category 3: Grades 7-8 Practice PaperPrum vattanakNo ratings yet
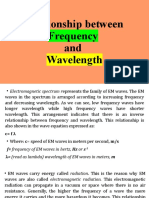
- LESSON 2. Calculating Wavelengtdytrjycghh and FrequencyDocument37 pagesLESSON 2. Calculating Wavelengtdytrjycghh and FrequencyRyan Aint simpNo ratings yet
- Column RevampsDocument10 pagesColumn RevampsChem.Engg100% (1)
- Agriculture For Engineers 1 PDFDocument267 pagesAgriculture For Engineers 1 PDFSagar SagwalNo ratings yet
- Earth and Life Quarter2 Week2 EDITEDDocument8 pagesEarth and Life Quarter2 Week2 EDITEDRandy montecalboNo ratings yet
- The Effects of A Nuclear Bomb PDFDocument2 pagesThe Effects of A Nuclear Bomb PDFThe Dangerous OneNo ratings yet
- Euroncap 2017 Dacia Duster DatasheetDocument15 pagesEuroncap 2017 Dacia Duster DatasheetmakkboyNo ratings yet
- Physico-Chemical Characterization of Distillery Effluent and Its Dilution Effect at Different LevelsDocument11 pagesPhysico-Chemical Characterization of Distillery Effluent and Its Dilution Effect at Different LevelsSiddu RhNo ratings yet
- LM160 LM360 High Speed Differential ComparatorDocument8 pagesLM160 LM360 High Speed Differential Comparatorradioscribd100% (1)
- Dna FingerprintingDocument13 pagesDna FingerprintingNaeem Khan Malizai100% (1)
- Book 4Document110 pagesBook 4pundirv1993No ratings yet
- Refrigeration and Air-Conditioning: Unit - 3Document30 pagesRefrigeration and Air-Conditioning: Unit - 3SAATVIK JAINNo ratings yet
- Contemporary Global GovernanceDocument11 pagesContemporary Global GovernanceLara Tessa VinluanNo ratings yet
- A One-Pot Synthesis of 3-Amino-3-Arylpropionic AcidsDocument13 pagesA One-Pot Synthesis of 3-Amino-3-Arylpropionic AcidsTuyenHHCNo ratings yet
- Nursing Memory JoggersDocument2 pagesNursing Memory JoggersMel Tabanao100% (1)
- Assignment-1 (2020011108)Document28 pagesAssignment-1 (2020011108)Atul KumarNo ratings yet
- Proposal For Improvement of Infant Toddler Weighing ScaleDocument6 pagesProposal For Improvement of Infant Toddler Weighing ScaleYuna-chan KatsuraNo ratings yet
- Monserrat, Patrick Reyes, Gwen Stefanie C. Robles, Daryl Tañada, Janine Kae Tancinco, Ashley Tininahan, Aliza MaeDocument2 pagesMonserrat, Patrick Reyes, Gwen Stefanie C. Robles, Daryl Tañada, Janine Kae Tancinco, Ashley Tininahan, Aliza Maegwen reyesNo ratings yet
- Speaker BiosDocument43 pagesSpeaker BiosAEHSFOUNDATIONNo ratings yet
- A Case Study of Google RecruitingDocument4 pagesA Case Study of Google Recruitingarunimajoy0% (1)
- Test Bank For Microbiology The Human Experience First Edition First EditionDocument15 pagesTest Bank For Microbiology The Human Experience First Edition First EditionSabina Moskowitz100% (6)
- IEC 60079-33 - Equipment Protection by Special Protection 'S' - Edition 1.0 - 2012Document42 pagesIEC 60079-33 - Equipment Protection by Special Protection 'S' - Edition 1.0 - 2012Institute of Marketing & Training ALGERIANo ratings yet
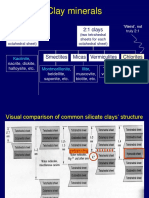
- 2 Silika Clay-1Document22 pages2 Silika Clay-1Anisa Ingin Clalu TersenyumNo ratings yet
- Medical Gas OutletsDocument48 pagesMedical Gas OutletsIrvin Bradford Dee100% (1)
- Sealing Technology June 2015Document16 pagesSealing Technology June 2015daniel.skydog1562No ratings yet
- Ensci 1100Document2 pagesEnsci 1100Zester MabasaNo ratings yet
- Araneta V GatmaitanDocument1 pageAraneta V GatmaitanJohn BasNo ratings yet
- HRM Case Studies CataloguesDocument13 pagesHRM Case Studies CataloguesMohamed alavianNo ratings yet