You might also like
- Ulcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryDocument71 pagesUlcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryFachry Al RafiqiNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Adrenal Insufficiency and Addison's DiseaseDocument8 pagesAdrenal Insufficiency and Addison's DiseaseyancefinceNo ratings yet
- Immune System. It's Possible That A Virus or Bacterium May Trigger Crohn's DiseaseDocument11 pagesImmune System. It's Possible That A Virus or Bacterium May Trigger Crohn's DiseaseZulfiana RahayuNo ratings yet
- Case Study PneumoniaDocument14 pagesCase Study PneumoniaJester GalayNo ratings yet
- Leukemia (: American English British English Cancer Blood Bone Marrow White Blood Cells BlastsDocument7 pagesLeukemia (: American English British English Cancer Blood Bone Marrow White Blood Cells BlastsArulmani MurugesanNo ratings yet
- Graves' Disease: Bella I. Putri 16-025Document29 pagesGraves' Disease: Bella I. Putri 16-025anon_414347743No ratings yet
- UTIDocument53 pagesUTIMimi Suhaini SudinNo ratings yet
- Leukemia StudyDocument18 pagesLeukemia StudyaneeshdNo ratings yet
- Pathophysiology of Arteriosclerosis and AtherosclerosisDocument22 pagesPathophysiology of Arteriosclerosis and Atherosclerosisjoyrena ochondraNo ratings yet
- Lupus NephritisDocument29 pagesLupus NephritisMuhammad Julpian0% (1)
- UtiDocument38 pagesUtiAzra AzmunaNo ratings yet
- Infra-Auricular Mass Case PresDocument8 pagesInfra-Auricular Mass Case PresEjay Jacob RicamaraNo ratings yet
- Cardiology Case 1Document2 pagesCardiology Case 1vil62650% (2)
- Diagnosis of Gastrointestinal Bleeding in AdultsDocument8 pagesDiagnosis of Gastrointestinal Bleeding in AdultsSaeed Al-YafeiNo ratings yet
- Pathophysiology of Heart FailureDocument2 pagesPathophysiology of Heart FailureJaysellePuguonTabijeNo ratings yet
- Are Viruses Living or Non-Living Organisms?Document8 pagesAre Viruses Living or Non-Living Organisms?Sydney Cloyce NagalNo ratings yet
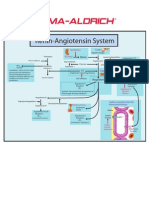
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Laboratory Diagnosis and Monitoring of Diabetes MellitusDocument65 pagesLaboratory Diagnosis and Monitoring of Diabetes MellitusSonia Afika AzizaNo ratings yet
- Myeloid LeukemiaDocument8 pagesMyeloid LeukemiaMiriam AguilarNo ratings yet
- Mechanism of HypertensionDocument4 pagesMechanism of HypertensionAlya Putri KhairaniNo ratings yet
- Congestive Heart FailureDocument64 pagesCongestive Heart FailureBentoys StreetNo ratings yet
- Acute Respiratory Distress SyndromeDocument20 pagesAcute Respiratory Distress SyndromeAngel Cauilan100% (1)
- Celiac Disease FinalDocument7 pagesCeliac Disease FinalacholineNo ratings yet
- Primary SyphilisDocument3 pagesPrimary SyphilisEqah TajuddinNo ratings yet
- Hanson Infectious Diseases - Anamneza I StatusDocument33 pagesHanson Infectious Diseases - Anamneza I StatusSilvia KesegNo ratings yet
- Chronic Myeloid LeukemiaDocument7 pagesChronic Myeloid LeukemiahemendreNo ratings yet
- Nuero ICHDocument20 pagesNuero ICHLINDSLEY GO100% (1)
- Pathophysiology PneumoniaDocument2 pagesPathophysiology PneumoniaChiro Rouy Malaluan100% (2)
- What Is HyperlipidemiaDocument9 pagesWhat Is Hyperlipidemiaichanara100% (2)
- Hepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisDocument3 pagesHepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisThuan Tăng NguyenNo ratings yet
- Immuno Modulator SDocument62 pagesImmuno Modulator SAntony Prakash RajNo ratings yet
- Book Cardio ConceptDocument29 pagesBook Cardio ConceptJulia Rae Delos SantosNo ratings yet
- Crohn's DiseaseDocument38 pagesCrohn's Diseasetintukmathew100% (1)
- Diabetes Mellitus Type 2Document16 pagesDiabetes Mellitus Type 2MTs MIFDANo ratings yet
- CompleteBloodCounts NORMAL VALUEDocument4 pagesCompleteBloodCounts NORMAL VALUEWoro Hapsari Wahyuningrum100% (1)
- A Case of A 61/M Client With Upper Gastrointestinal Bleeding Secondary To Peptic Ulcer DiseaseDocument3 pagesA Case of A 61/M Client With Upper Gastrointestinal Bleeding Secondary To Peptic Ulcer DiseasejohndavennarvaezNo ratings yet
- TB TreatmentDocument58 pagesTB TreatmentNdayisaba CorneilleNo ratings yet
- LeukemiaDocument15 pagesLeukemiaShashidhar K Bangera100% (1)
- Pathophysiology of DiseaseDocument7 pagesPathophysiology of DiseaseYannah Mae EspineliNo ratings yet
- Pathophysiology of SepsisDocument8 pagesPathophysiology of SepsisntnquynhproNo ratings yet
- Leptospirosis FinalDocument5 pagesLeptospirosis FinalufrieNo ratings yet
- Drug Induced NephrotoxicityDocument13 pagesDrug Induced NephrotoxicityAgnes BastonNo ratings yet
- Antihyperglycemic Agents Comparison ChartDocument9 pagesAntihyperglycemic Agents Comparison ChartBonnieNo ratings yet
- Rabies: Ragina AguilaDocument55 pagesRabies: Ragina AguilaCharles Lester AdalimNo ratings yet
- Laboratory Results or Findings CholeDocument3 pagesLaboratory Results or Findings CholecookiemonsterlyNo ratings yet
- 18 IM 3.02 Systemic Lupus ErythematosusDocument8 pages18 IM 3.02 Systemic Lupus ErythematosusKaykie CalambaNo ratings yet
- Physical Inactivity: Aging Men Hypertension Smoker ObesityDocument1 pagePhysical Inactivity: Aging Men Hypertension Smoker ObesityKEn PilapilNo ratings yet
- Ulcerative ColitisDocument8 pagesUlcerative ColitispipotoNo ratings yet
- Liver Cirosis Case StudyDocument18 pagesLiver Cirosis Case StudyDaniel LaurenteNo ratings yet
- EBM - 5. Adrenal DisordersDocument101 pagesEBM - 5. Adrenal DisordersBRI KUNo ratings yet
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNo ratings yet
- DB13 - Pathophysiology of AtherosclerosisDocument2 pagesDB13 - Pathophysiology of Atherosclerosisi_vhie03No ratings yet
- Myasthenia Gravis Case Study 01Document3 pagesMyasthenia Gravis Case Study 01PJHG0% (1)
- Case Study 52 Cushing SyndromeDocument4 pagesCase Study 52 Cushing SyndromeAnonymous G7AdqnemziNo ratings yet
- GastroenteritisDocument3 pagesGastroenteritisNicoleNo ratings yet
- Clinical Scenario and Worksheet For Diagnostic Appraisal (Journal On Dengue)Document3 pagesClinical Scenario and Worksheet For Diagnostic Appraisal (Journal On Dengue)Stephie E.No ratings yet
- Disease EssayDocument5 pagesDisease Essayapi-309393081No ratings yet
- Normal Values of CBCDocument1 pageNormal Values of CBCCherr NollNo ratings yet
- Ulcerative ColitisDocument12 pagesUlcerative Colitisthap87No ratings yet
- Pelvic Floor MuscleDocument11 pagesPelvic Floor MuscleSonia guptaNo ratings yet
- TEP 2, Thera Ex 1 and Physiology 2 SyllabusDocument2 pagesTEP 2, Thera Ex 1 and Physiology 2 SyllabusJohnpeter EsporlasNo ratings yet
- Halo Sport User ManualDocument18 pagesHalo Sport User ManualMuhammad Addinul Huda100% (1)
- Cardiotonic Drugs Revised DheryanDocument16 pagesCardiotonic Drugs Revised Dheryanlinnet17No ratings yet
- %pecta (: P'erfectedDocument5 pages%pecta (: P'erfectedjuan perez arrikitaunNo ratings yet
- N, M, M: A M M - B H: Research LetterDocument9 pagesN, M, M: A M M - B H: Research LetterOlivier BenarrocheNo ratings yet
- Oral Lec 8Document9 pagesOral Lec 8Adam AliraqiNo ratings yet
- Post-Transcriptional ModificationDocument20 pagesPost-Transcriptional ModificationZain YaqoobNo ratings yet
- Patel 2014Document7 pagesPatel 2014Javiera Munizaga MuñozNo ratings yet
- Science 10 3rd Quarter Exam - PDF - Messenger Rna - RibosomeDocument1 pageScience 10 3rd Quarter Exam - PDF - Messenger Rna - RibosomeKedir MohammedNo ratings yet
- Science 6 - Week 4 - 2nd QuarterDocument5 pagesScience 6 - Week 4 - 2nd QuarterHoneylet Alberto Castro ArilloNo ratings yet
- Enteric Nervous SystemDocument12 pagesEnteric Nervous SystemedgarNo ratings yet
- Common Board QuestionDocument17 pagesCommon Board QuestionJonathan Renier VerzosaNo ratings yet
- MEDI7112 GIT Lecture Checklist 2015Document2 pagesMEDI7112 GIT Lecture Checklist 2015zjaffri89No ratings yet
- Ex3 PostLabDocument4 pagesEx3 PostLabDaniel Seth AndalNo ratings yet
- (Physio A) ECG (Javier)Document4 pages(Physio A) ECG (Javier)AliNo ratings yet
- Autopsy ReportDocument9 pagesAutopsy ReportHank LeeNo ratings yet
- Respiratory Examination - Protected 1Document4 pagesRespiratory Examination - Protected 1anirudh811100% (1)
- Davis's NCLEX-RN® Success 3E (2012) - MEMORY AIDS - IMPORTANTDocument4 pagesDavis's NCLEX-RN® Success 3E (2012) - MEMORY AIDS - IMPORTANTMaria Isabel Medina MesaNo ratings yet
- 8.aviation, Space and Deep Sea Diving PhysiologyDocument5 pages8.aviation, Space and Deep Sea Diving PhysiologyCLEMENTNo ratings yet
- Reports 2Document10 pagesReports 2Tejaswini ReddyNo ratings yet
- Common Diseases of NewbornDocument162 pagesCommon Diseases of NewbornMichelle ThereseNo ratings yet
- List of Medical Roots, Suffixes and Prefixes - Wikipedia, The Free EncyclopediaDocument35 pagesList of Medical Roots, Suffixes and Prefixes - Wikipedia, The Free EncyclopediaHoward GouldNo ratings yet
- tmp4946 TMPDocument27 pagestmp4946 TMPFrontiersNo ratings yet
- AP1 Lab4 Intro To Skeleton FA2021Document15 pagesAP1 Lab4 Intro To Skeleton FA2021Kim VenturaNo ratings yet
- Extension Worksheet - Option HDocument2 pagesExtension Worksheet - Option HHellö PëachNo ratings yet
- Risk For Aspiration Nursing Care PlanDocument6 pagesRisk For Aspiration Nursing Care PlanWendy Escalante100% (3)
- Neural EngineeringDocument377 pagesNeural Engineeringbeesah100% (1)
- BISC403 Sample Exam 4 W - Answers 20SpDocument5 pagesBISC403 Sample Exam 4 W - Answers 20SpGrace MillsNo ratings yet
- Anatomy and Physiology of Respiratory System Tutorial2Document1 pageAnatomy and Physiology of Respiratory System Tutorial2Jhullian Frederick Val VergaraNo ratings yet