You might also like
- Joint Structure and FunctionDocument87 pagesJoint Structure and Functionjay shah90% (21)
- Call of Cthulhu - The Arkham Gazette #3 (7E Conversion)Document20 pagesCall of Cthulhu - The Arkham Gazette #3 (7E Conversion)tommy fletcher100% (2)
- Biology of Tendon Injury: Healing, Modeling and Remodeling: P. Sharma and N. MaffulliDocument10 pagesBiology of Tendon Injury: Healing, Modeling and Remodeling: P. Sharma and N. MaffulliBrianna RyanNo ratings yet
- Tendon Injuries - EFORT Open ReviewsDocument23 pagesTendon Injuries - EFORT Open ReviewsAvram GeorgievNo ratings yet
- Tendon Structure and HealingDocument9 pagesTendon Structure and HealingLuki ErtandriNo ratings yet
- Tendon Injury and Tendinopathy: Healing and Repair: Current Concepts ReviewDocument16 pagesTendon Injury and Tendinopathy: Healing and Repair: Current Concepts ReviewNicolas ParejaNo ratings yet
- Jbjs Tendonopathy Tendinosis Healing RepairDocument17 pagesJbjs Tendonopathy Tendinosis Healing RepairPauloNo ratings yet
- Histopathology of Common TendinopathiesDocument18 pagesHistopathology of Common TendinopathiesJulieta DiyorioNo ratings yet
- Collagen StructureDocument17 pagesCollagen StructureMontserrat LandaNo ratings yet
- Describe The Material Properties of Articular Connective TissueDocument4 pagesDescribe The Material Properties of Articular Connective TissueAyhan AbdulAzizNo ratings yet
- Common Tendinopathies in The Upper and LDocument10 pagesCommon Tendinopathies in The Upper and LVladislav KotovNo ratings yet
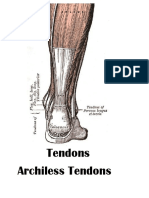
- TendonsDocument35 pagesTendonsMaricris Alison Kabiling ElauriaNo ratings yet
- BR Med Bull 2011 Sakabe BMB Ldr025Document15 pagesBR Med Bull 2011 Sakabe BMB Ldr025VersoNo ratings yet
- Disk DegenDocument25 pagesDisk DegenLaviniaBrănescuNo ratings yet
- Tendon and Ligament Healing and Current Approaches To Tendon and Ligament RegenerationDocument6 pagesTendon and Ligament Healing and Current Approaches To Tendon and Ligament RegenerationQUIRA VANESSA SALAZAR JIMENEZNo ratings yet
- Engineering in Medicine 5 NotesDocument110 pagesEngineering in Medicine 5 NotesDaniel Montilla NavasNo ratings yet
- Aaos OkuDocument752 pagesAaos OkuJoao Vide100% (5)
- Pain in OsteoarthritisDocument24 pagesPain in OsteoarthritisTania Garcia MollNo ratings yet
- Ligament Structure, Physiology and FunctionDocument3 pagesLigament Structure, Physiology and FunctionTyler Latu'ilaNo ratings yet
- Patogenese TendõesDocument15 pagesPatogenese TendõesRenan O. Pravatta PivettaNo ratings yet
- TMJ AnatomyDocument68 pagesTMJ AnatomyArchanaShenoyNo ratings yet
- Tissue Biochemistry ChapterDocument25 pagesTissue Biochemistry ChapterMaria ArshadNo ratings yet
- 46 MusclesDocument5 pages46 Musclesuddim004100% (2)
- Biomechanics of Soft Tissue: Biomech Preprint SeriesDocument15 pagesBiomechanics of Soft Tissue: Biomech Preprint Seriesaloove66No ratings yet
- Estructura y Composición Del TendónDocument8 pagesEstructura y Composición Del TendónCelia DizNo ratings yet
- A Comparison of MRI and US Findings in Tendinosis: Christina VongDocument27 pagesA Comparison of MRI and US Findings in Tendinosis: Christina VongChristina VongNo ratings yet
- 2016 10 18 The Extracellular Matrix (ECM)Document45 pages2016 10 18 The Extracellular Matrix (ECM)sennaavia12100% (1)
- Biomechanics of CartilageDocument15 pagesBiomechanics of CartilageMandestt MergiyawNo ratings yet
- Muscle Fascia and Force Transmission: Peter P. Purslow, PHDDocument7 pagesMuscle Fascia and Force Transmission: Peter P. Purslow, PHDBangun MakmunNo ratings yet
- Biochemistry of Integumen, Dr. Tisna Sendy PDocument65 pagesBiochemistry of Integumen, Dr. Tisna Sendy PrismaorchitaNo ratings yet
- Biomechanics of Muscle (Skeletal)Document19 pagesBiomechanics of Muscle (Skeletal)Murad KurdiNo ratings yet
- Histologi Jaringan Kartilago - FK UNSRIDocument16 pagesHistologi Jaringan Kartilago - FK UNSRIRSatriaSuryaCandraNo ratings yet
- Add InfoDocument5 pagesAdd InfoWestminster AbbeyNo ratings yet
- Medicina 55 00447Document12 pagesMedicina 55 00447ChawNo ratings yet
- CytoskeletonDocument9 pagesCytoskeletonGordon YapNo ratings yet
- Textus ConnectivusDocument43 pagesTextus ConnectivusShafiraNo ratings yet
- Biomechanical Properties of Cartilage: Mr. Jignesh Dhamelia Ii-MptDocument27 pagesBiomechanical Properties of Cartilage: Mr. Jignesh Dhamelia Ii-MptdeepuphysioNo ratings yet
- Cartilage Supplement, Vitamins, Herbs, Natural Ways To Improve and To Have Healthy TissueDocument5 pagesCartilage Supplement, Vitamins, Herbs, Natural Ways To Improve and To Have Healthy TissueSN WijesinheNo ratings yet
- MusclesssDocument4 pagesMusclesssLiam Jacque LapuzNo ratings yet
- Advanced Anatomy - Myofascial MeridiansDocument37 pagesAdvanced Anatomy - Myofascial MeridiansBioTaoQi100% (2)
- Connective TissuesDocument10 pagesConnective Tissuesbenishgulzar50No ratings yet
- Basic Science of Articular Cartilage and Osteoarthritis: Andrew D. Pearle, MD, Russell F. Warren, MD, Scott A. Rodeo, MDDocument12 pagesBasic Science of Articular Cartilage and Osteoarthritis: Andrew D. Pearle, MD, Russell F. Warren, MD, Scott A. Rodeo, MDNantini GopalNo ratings yet
- BetterOrthopedics 2nd-EdLesondak ChapterDocument12 pagesBetterOrthopedics 2nd-EdLesondak Chapter施凯No ratings yet
- Case Study LypotDocument16 pagesCase Study LypotlyrenangelicaNo ratings yet
- Ijms 21 00844 v3Document20 pagesIjms 21 00844 v3Jose PerezNo ratings yet
- Vet Histo Notes Chap 3Document15 pagesVet Histo Notes Chap 3Mia Kristhyn Calinawagan SabanalNo ratings yet
- Ten Dinos IsDocument9 pagesTen Dinos IsIsa Cahya permadiNo ratings yet
- The Effect of Mechanical Loading On Articular Cartilage: Giuseppe MusumeciDocument8 pagesThe Effect of Mechanical Loading On Articular Cartilage: Giuseppe MusumeciMani RajNo ratings yet
- 4.1 CytoskeletonDocument28 pages4.1 Cytoskeletonedabzan234No ratings yet
- Connective Tissue: Group MembersDocument28 pagesConnective Tissue: Group MembersIkhsan HidayatNo ratings yet
- 1.2 Cartilage and BoneDocument27 pages1.2 Cartilage and BonePema GaleyNo ratings yet
- المستندDocument7 pagesالمستندمحمود محمدNo ratings yet
- Chapter - 3 Life Processes-Movement in Animals and PlantsDocument15 pagesChapter - 3 Life Processes-Movement in Animals and PlantsArchanna VyassNo ratings yet
- Tendon Cells Root Into (Instead of Attach To) Humeral Bone Head Via Fibrocartilage-EnthesisDocument21 pagesTendon Cells Root Into (Instead of Attach To) Humeral Bone Head Via Fibrocartilage-EnthesisНадія АсадуллаєваNo ratings yet
- Chronic Tendon Pathology: Molecular Basis and Therapeutic ImplicationsDocument25 pagesChronic Tendon Pathology: Molecular Basis and Therapeutic ImplicationsMuñoz Cerón Smiht YhoissNo ratings yet
- Disability & Rehabilitation Volume 23 issue 13 2001 [doi 10.1080%2F09638280010029930] James, S. E. Farmer, M. -- Contractures in orthopaedic and neurological conditions- a review of causes and treatme (1).pdfDocument10 pagesDisability & Rehabilitation Volume 23 issue 13 2001 [doi 10.1080%2F09638280010029930] James, S. E. Farmer, M. -- Contractures in orthopaedic and neurological conditions- a review of causes and treatme (1).pdfMensah Yao AmedzoNo ratings yet
- Tugas Self Directed Learning Sains Dan Biomedik DasarDocument7 pagesTugas Self Directed Learning Sains Dan Biomedik DasarApria PratamaNo ratings yet
- Skeletal Muscle Contraction and The Motor UnitsDocument4 pagesSkeletal Muscle Contraction and The Motor UnitsAnonymous vnv6QFNo ratings yet
- Biology Lecture Notes: (Stemer'S Guide)Document16 pagesBiology Lecture Notes: (Stemer'S Guide)Ahmed KamelNo ratings yet
- Advanced farriery knowledge: A study guide and AWCF theory course companionFrom EverandAdvanced farriery knowledge: A study guide and AWCF theory course companionNo ratings yet
- Hemichordata and Invertebrate ChordatesDocument31 pagesHemichordata and Invertebrate ChordatesayonNo ratings yet
- Para Sample QuestionsDocument5 pagesPara Sample QuestionsMaria Christina LagartejaNo ratings yet
- Clostridium and MycobacteriumDocument40 pagesClostridium and MycobacteriumSAYMABANUNo ratings yet
- LEAPS Fugl-Meyer InstructionsDocument17 pagesLEAPS Fugl-Meyer InstructionsDaniele Bertolo100% (1)
- Retention and Relapse PDFDocument4 pagesRetention and Relapse PDFFernaz BehlimNo ratings yet
- Strongyloidiasis: Etiology: Strongyloides StercoralisDocument20 pagesStrongyloidiasis: Etiology: Strongyloides StercoralisnusriniNo ratings yet
- Anatomy & Physiology - AllDocument15 pagesAnatomy & Physiology - AllAnubhav ShuklaNo ratings yet
- Tetralogy of FallotDocument33 pagesTetralogy of FallotjeenaejyNo ratings yet
- Dr. P. SAthiyarajeswaran - Suvai (Taste) and Uyir Thathu (2018Document12 pagesDr. P. SAthiyarajeswaran - Suvai (Taste) and Uyir Thathu (2018Vishnu Prabhu SivasubramaniamNo ratings yet
- Risk Management Prelim ReviewerDocument3 pagesRisk Management Prelim ReviewerCharmaigne BañaresNo ratings yet
- MaternityDocument91 pagesMaternityAnonymous D8KswoNo ratings yet
- Quiz ReproductiveDocument78 pagesQuiz ReproductiveMedShare86% (7)
- Beginner's Guide To Getting Started With DiscusDocument18 pagesBeginner's Guide To Getting Started With DiscusGary HoustonNo ratings yet
- Hamster Biology HusbandryDocument39 pagesHamster Biology HusbandryKulenović Zlatan100% (1)
- Tula at Reviewer For PrintDocument14 pagesTula at Reviewer For PrintMariejho GensayaNo ratings yet
- Ad&d The Book of Lairs IIDocument97 pagesAd&d The Book of Lairs IIJohn Strickler100% (7)
- Digestive System AnatomyDocument8 pagesDigestive System AnatomyBrittany Lei MaquirayaNo ratings yet
- Effects of Bimanual Functional Practice Training On Functional Performance of Upper Extremity in Chronic Stroke SRJI Vol 2 Issue 3 Year 2013Document10 pagesEffects of Bimanual Functional Practice Training On Functional Performance of Upper Extremity in Chronic Stroke SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNo ratings yet
- Advanced Guide To Chakra and Charts V17Document34 pagesAdvanced Guide To Chakra and Charts V17Magia Del Mar100% (2)
- Specimen Collection, Transport and ProcessingDocument29 pagesSpecimen Collection, Transport and ProcessingGladys Marie WillkomNo ratings yet
- RehumaticDocument3 pagesRehumaticgopscharanNo ratings yet
- Nodal Stations of The AbdomenDocument8 pagesNodal Stations of The Abdomenborst0% (1)
- Pathology, Lecture 6 (Lecture Notes)Document18 pagesPathology, Lecture 6 (Lecture Notes)Ali Al-Qudsi100% (1)
- Daftar PustakaDocument3 pagesDaftar PustakaicaNo ratings yet
- Tahir G CV UpdateDocument5 pagesTahir G CV UpdateTahir GeradNo ratings yet
- 2.biomekanik Pada Edentulus PenuhDocument27 pages2.biomekanik Pada Edentulus PenuhJesica Dwiasta Octaria NainggolanNo ratings yet
- Hubungan Antara Nilai Hematokrit Dengan Trombosit Terhadap Hasil Pemeriksaan Ns1 Dan Serologi Igm Dan Igg Pada Pasien Demam Berdarah DengueDocument7 pagesHubungan Antara Nilai Hematokrit Dengan Trombosit Terhadap Hasil Pemeriksaan Ns1 Dan Serologi Igm Dan Igg Pada Pasien Demam Berdarah DengueHaidar HanifNo ratings yet
- Duck Rearing and ManagemntDocument49 pagesDuck Rearing and Managemntkaranpraba1901No ratings yet
- Cornell Note TakingDocument2 pagesCornell Note Takingapi-254514513No ratings yet





















































![Disability & Rehabilitation Volume 23 issue 13 2001 [doi 10.1080%2F09638280010029930] James, S. E. Farmer, M. -- Contractures in orthopaedic and neurological conditions- a review of causes and treatme (1).pdf](https://imgv2-1-f.scribdassets.com/img/document/254019242/149x198/9467d687df/1422478524?v=1)