You might also like
- RegistrationDocument4 pagesRegistrationruksfarhanNo ratings yet
- Rajasthan Medical Council: Sardar Patel Marg, C-Scheme, Jaipur-302001Document4 pagesRajasthan Medical Council: Sardar Patel Marg, C-Scheme, Jaipur-302001KaushalGoyal0% (1)
- FORM 1 (Registration)Document4 pagesFORM 1 (Registration)Suraj PathakNo ratings yet
- Internship FORM (PT)Document2 pagesInternship FORM (PT)Tanya SharmaNo ratings yet
- Permanent FormDocument4 pagesPermanent FormdgfuiNo ratings yet
- The Model Letter of Willingness From A Voluntary Body DonorDocument4 pagesThe Model Letter of Willingness From A Voluntary Body DonorBalaji VenkataramanNo ratings yet
- Foreign Provisional Permenant RegistrationDocument11 pagesForeign Provisional Permenant RegistrationTina ThomsonNo ratings yet
- MesdkjlDocument6 pagesMesdkjlRahul KirkNo ratings yet
- Reg FormDocument2 pagesReg Formdr.drpatilNo ratings yet
- Haryana Medical Council registration formsDocument13 pagesHaryana Medical Council registration formsANCIENT MYSTERIES OF THE WORLDNo ratings yet
- BHPC Application Form For Penn Updated Jan 2019Document6 pagesBHPC Application Form For Penn Updated Jan 2019sosomiso234No ratings yet
- Death Claimant StatementDocument4 pagesDeath Claimant Statementcet.ranchi7024No ratings yet
- Travancore-Cochin Council of Indian Systems of MedicineDocument2 pagesTravancore-Cochin Council of Indian Systems of MedicineDr Thushar T.SNo ratings yet
- General Circular For MD October, 2022Document18 pagesGeneral Circular For MD October, 2022akhilNo ratings yet
- Sicknessandfitnesscertificates PDFDocument6 pagesSicknessandfitnesscertificates PDFniraj_sdNo ratings yet
- All Annexure 3,7,8,9,10Document5 pagesAll Annexure 3,7,8,9,10prafful_hereNo ratings yet
- Form4 Provisional MMCDocument3 pagesForm4 Provisional MMCminci sensei100% (2)
- Application Form For Contract Medical Officer (Non - Citizens) PDFDocument19 pagesApplication Form For Contract Medical Officer (Non - Citizens) PDFHafiz IbrahimNo ratings yet
- Provisional RegistrationDocument9 pagesProvisional RegistrationabuprettyNo ratings yet
- Apply Good Standing Certificate Travancore-Coch Medical CouncilsDocument2 pagesApply Good Standing Certificate Travancore-Coch Medical Councilslife connectNo ratings yet
- Form of Application For Registration of Dentist Under Section 34 of The Dentists Act, 1948 (XVI of 1948)Document5 pagesForm of Application For Registration of Dentist Under Section 34 of The Dentists Act, 1948 (XVI of 1948)vijai gasNo ratings yet
- Application Foreign NationalsDocument7 pagesApplication Foreign NationalsKaranGargNo ratings yet
- Application FormDocument2 pagesApplication FormRajat SharmaNo ratings yet
- Tue Application FormDocument4 pagesTue Application FormHengky AntonNo ratings yet
- Renewal Homoeo Form 2019Document2 pagesRenewal Homoeo Form 2019deepa rNo ratings yet
- Application Form For TCHPDocument6 pagesApplication Form For TCHPDean E&T SRM IST TrichyNo ratings yet
- Body Donation Pledge Format EnglishDocument7 pagesBody Donation Pledge Format Englishlingegowda naanuNo ratings yet
- Not 0042022 0942022Document5 pagesNot 0042022 0942022anoop616No ratings yet
- The Will Form For Donation of Body After Death: Hundred .Document2 pagesThe Will Form For Donation of Body After Death: Hundred .Andrew VincentNo ratings yet
- agra DH jhegbcddDocument20 pagesagra DH jhegbcddPrdptiwariNo ratings yet
- Statutory Declaration FormDocument3 pagesStatutory Declaration Formmackcaslangan08No ratings yet
- DBDocument5 pagesDBJo JsNo ratings yet
- Admissio N Form-2011: For Mbbs/Bds in Medical/Dental Colleges of RajasthanDocument11 pagesAdmissio N Form-2011: For Mbbs/Bds in Medical/Dental Colleges of RajasthanJitendra ChoudharyNo ratings yet
- IIVMembership PDFDocument2 pagesIIVMembership PDFdvNo ratings yet
- BDS Application FormDocument3 pagesBDS Application FormPrasad SrbNo ratings yet
- Registration FormDocument8 pagesRegistration FormNitin Kashyap0% (1)
- MEDICAL CERTIFICATE FOR INTELLIGENCE BUREAUDocument13 pagesMEDICAL CERTIFICATE FOR INTELLIGENCE BUREAUnidhi sharmaNo ratings yet
- Death Claim Form - Ashx PDFDocument7 pagesDeath Claim Form - Ashx PDFqaiserjamshedNo ratings yet
- Spot & MQ ApplicationDocument2 pagesSpot & MQ Applicationbhagathi nageswara raoNo ratings yet
- Indian Passport Application - Form 2Document8 pagesIndian Passport Application - Form 2saruljainNo ratings yet
- Advertisement For Paramedical StaffsDocument4 pagesAdvertisement For Paramedical Staffssatyajitmishra2009No ratings yet
- SC Health and Welfare FormDocument4 pagesSC Health and Welfare FormLeandro Tamayo14% (7)
- Good StandingDocument2 pagesGood StandingruksfarhanNo ratings yet
- Not 0092021 2142021Document5 pagesNot 0092021 2142021ഹിന്ദുNo ratings yet
- Application Form For Local EN EngDocument1 pageApplication Form For Local EN EngYing Ying CHEUNGNo ratings yet
- Post Basic FormDocument6 pagesPost Basic FormAyush MewaraNo ratings yet
- Application FormDocument8 pagesApplication FormMafruha AfrinNo ratings yet
- Check List For Joining: Phulwarisharif, Patna-801507Document32 pagesCheck List For Joining: Phulwarisharif, Patna-801507Ashutosh SinghNo ratings yet
- Railway Hospital FormDocument1 pageRailway Hospital Formmanum8No ratings yet
- Eligibility Certificate PDFDocument10 pagesEligibility Certificate PDFManoj PeddintiNo ratings yet
- SPL Edn Form DT 18042019 PDFDocument10 pagesSPL Edn Form DT 18042019 PDFSoniaNo ratings yet
- Check List For Mbbs Admission-2020: (Documents Shall Be Arranged in The Following Order)Document8 pagesCheck List For Mbbs Admission-2020: (Documents Shall Be Arranged in The Following Order)manoj DocsNo ratings yet
- Anna University: Chennai-600 025, IndiaDocument12 pagesAnna University: Chennai-600 025, IndiaMAX PAYNENo ratings yet
- Paramedical Council Registration ApplicationDocument3 pagesParamedical Council Registration ApplicationNouri gafoorNo ratings yet
- Consent FormDocument1 pageConsent FormJun Huan WongNo ratings yet
- SLMC GoodstandingDocument2 pagesSLMC GoodstandingTharaka NuwanNo ratings yet
- DU Law Faculty Application FormDocument3 pagesDU Law Faculty Application Formvishnu gopakumarNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- Manual on the Character and Fitness Process for Application to the Michigan State Bar: Law and PracticeFrom EverandManual on the Character and Fitness Process for Application to the Michigan State Bar: Law and PracticeNo ratings yet
- New York Notary Public Prep Book with 3 Full Practice TestsFrom EverandNew York Notary Public Prep Book with 3 Full Practice TestsRating: 5 out of 5 stars5/5 (2)
- Chemistry in Everyday LifeDocument33 pagesChemistry in Everyday LifeArya StarkNo ratings yet
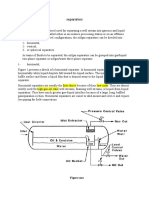
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- BiostastisticDocument2 pagesBiostastisticاحمد ماجد زبنNo ratings yet
- Detailed Lesson Plan in Household Services Adiel RavaneraDocument8 pagesDetailed Lesson Plan in Household Services Adiel RavaneraAdielNo ratings yet
- Journal Titles and DetailsDocument30 pagesJournal Titles and DetailsMinerva Medical Treatment Pvt LtdNo ratings yet
- Pharmaceutical Microbiology - B.pharmDocument383 pagesPharmaceutical Microbiology - B.pharmkeyurNo ratings yet
- Ramial Chipped Wood - A Basic Tool For Regenerating SoilsDocument15 pagesRamial Chipped Wood - A Basic Tool For Regenerating SoilsmrmiscNo ratings yet
- ป 6Document43 pagesป 6MoLo Kanyarat ChenpitaksombatNo ratings yet
- ANPATH1 ReviewerDocument17 pagesANPATH1 ReviewerRashid DayaoNo ratings yet
- MFT28 - Greg Plitt's 4-Week Military Fitness Trainer by MET-RxDocument7 pagesMFT28 - Greg Plitt's 4-Week Military Fitness Trainer by MET-RxRayNo ratings yet
- Chap 24 Econ 40Document4 pagesChap 24 Econ 40Racel DelacruzNo ratings yet
- Girl Scouts ActivitiesDocument5 pagesGirl Scouts ActivitiessluttybitchNo ratings yet
- Different Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowDocument6 pagesDifferent Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowMadhuchandra HirehalliNo ratings yet
- Answers To Extra PracticeDocument5 pagesAnswers To Extra PracticesaraNo ratings yet
- Bibliometric Handbook For Karolinska InstitutetDocument41 pagesBibliometric Handbook For Karolinska InstitutetCamila Araya G100% (1)
- NAVAL Hot Tapping Tool User GuideDocument19 pagesNAVAL Hot Tapping Tool User GuidemarconelucenapereiraNo ratings yet
- Color Me VeganDocument272 pagesColor Me VeganBela Luísa Novo100% (1)
- Shell Turbo T32: Performance, Features & Benefits Main ApplicationsDocument3 pagesShell Turbo T32: Performance, Features & Benefits Main ApplicationsPandu SatrioNo ratings yet
- Separation Processes Lecture 1 IntroductionDocument14 pagesSeparation Processes Lecture 1 Introductionabood assrfndyNo ratings yet
- Psychedelic Drugs-A New Era in Psychiatry?Document9 pagesPsychedelic Drugs-A New Era in Psychiatry?PeterNo ratings yet
- BW Mc2 XWHM y Na ManualDocument23 pagesBW Mc2 XWHM y Na ManualSatyasrinivas PulavarthiNo ratings yet
- Automated Hematology Cell Counters 12-09-2023Document161 pagesAutomated Hematology Cell Counters 12-09-2023Tom JohnathanNo ratings yet
- General Conditions of Contracts For NLNG 2018Document28 pagesGeneral Conditions of Contracts For NLNG 2018AF Dowell MirinNo ratings yet
- SECTION 03380 Post-Tensioned Concrete Rev 1Document30 pagesSECTION 03380 Post-Tensioned Concrete Rev 1Abdalrahman AntariNo ratings yet
- Alpine Valley Liability ReleaseDocument1 pageAlpine Valley Liability ReleaseChristina Nakazaki0% (1)
- Business Plan Hair DyeDocument12 pagesBusiness Plan Hair Dyercool_rahul0039341No ratings yet
- Zollinger-Ellison Syndrome (Gastrinoma)Document15 pagesZollinger-Ellison Syndrome (Gastrinoma)Huy QuangNo ratings yet
- Deliver VALUE and RENEWABLE FUTUREDocument30 pagesDeliver VALUE and RENEWABLE FUTUREAlexandru SuciuNo ratings yet
- UNSG Report On Safety Security Humanitarian PersonnelDocument25 pagesUNSG Report On Safety Security Humanitarian PersonnelInterAction100% (1)
- Erowid LSD (Acid) Vault - ImagesDocument2 pagesErowid LSD (Acid) Vault - ImagesAdam BruhNo ratings yet