You might also like
- Soalan IvDocument3 pagesSoalan IvNeach GaoilNo ratings yet
- Topic 3 - A Strategic Perspective - EDITEDDocument68 pagesTopic 3 - A Strategic Perspective - EDITEDmayjayNo ratings yet
- Fundamental Research Grant Scheme (FRGS) Application Form: Jabatan Pengajian Tinggi Kementerian Pengajian TinggiDocument12 pagesFundamental Research Grant Scheme (FRGS) Application Form: Jabatan Pengajian Tinggi Kementerian Pengajian TinggiZul-AtfiNo ratings yet
- 20160228110202L4 Induction and OrientationDocument23 pages20160228110202L4 Induction and Orientationچئڬوعيدال100% (1)
- Survey To Study The Relationship Between Motivation and Reward SystemsDocument3 pagesSurvey To Study The Relationship Between Motivation and Reward Systemsadel22No ratings yet
- ACC 106 Chapter 1Document13 pagesACC 106 Chapter 1Firdaus Yahaya100% (4)
- What Is A Stakeholder New NehaDocument10 pagesWhat Is A Stakeholder New NehaOmkar BansodeNo ratings yet
- Depression Proposal 2018Document17 pagesDepression Proposal 2018nur78100% (2)
- Chap - 6 Compensation ManagementDocument12 pagesChap - 6 Compensation ManagementshrikantNo ratings yet
- Role of Od Pract 1Document22 pagesRole of Od Pract 1rakesh24hrs100% (1)
- Apa Itu PenyeliaanDocument18 pagesApa Itu PenyeliaanAsrap PrimaveraNo ratings yet
- 6 Dimensions of Organizational CultureDocument2 pages6 Dimensions of Organizational CultureEstella Balubar BawalanNo ratings yet
- Code of Practice On The Prevention and Eradication of Sexual Harassment in The WorkplaceDocument13 pagesCode of Practice On The Prevention and Eradication of Sexual Harassment in The WorkplaceWilliam TeoNo ratings yet
- Factors Influencing Job Satisfaction Among Gen X and Gen YDocument10 pagesFactors Influencing Job Satisfaction Among Gen X and Gen YfirinaluvinaNo ratings yet
- Assignment Gelagat OrganisasiDocument19 pagesAssignment Gelagat Organisasiwilliam tangNo ratings yet
- Study On Delay Construction Project in IndiaDocument5 pagesStudy On Delay Construction Project in IndiaMahadeoNo ratings yet
- Research Proposal BehailuDocument14 pagesResearch Proposal BehailuAndinet50% (4)
- BPMN 3143 Research Methodology: Chapter 1: IntroductionDocument27 pagesBPMN 3143 Research Methodology: Chapter 1: Introductionlin808No ratings yet
- KPI: Kaedah Membina Dan Mengawal Untuk Organisasi AwamDocument103 pagesKPI: Kaedah Membina Dan Mengawal Untuk Organisasi AwammbustamanabdmanafNo ratings yet
- Staffing, Training, and Compensation For Global Operations: The Organizational ContextDocument4 pagesStaffing, Training, and Compensation For Global Operations: The Organizational ContextMakmur PanjaitanNo ratings yet
- Job DesignDocument19 pagesJob DesignJibesaNo ratings yet
- Elton Mayo Theory: DR Amit K Lal Founder SkillicsDocument9 pagesElton Mayo Theory: DR Amit K Lal Founder Skillicsimdad ullahNo ratings yet
- Research Case StudyDocument6 pagesResearch Case StudyTan Boon JinNo ratings yet
- Malaysia Quality of LifeDocument35 pagesMalaysia Quality of LifeAieyda Nazri100% (7)
- Elc Critical AnalysisDocument3 pagesElc Critical AnalysisafiqahanuwarNo ratings yet
- International Journal of Business and Management Studies Vol 4, No 2, 2012 ISSN: 1309-8047 (Online)Document12 pagesInternational Journal of Business and Management Studies Vol 4, No 2, 2012 ISSN: 1309-8047 (Online)Onyeka1234No ratings yet
- Motivation and Reward SystemDocument25 pagesMotivation and Reward SystemMark JedNo ratings yet
- Emami-Study On The Motivational Techniques (Final Project)Document57 pagesEmami-Study On The Motivational Techniques (Final Project)Sneha DebNo ratings yet
- Soal Selidik Stress ManualDocument27 pagesSoal Selidik Stress ManualAzura Ab RahmanNo ratings yet
- MGT321 Chapter 4Document3 pagesMGT321 Chapter 4AIZAT ALIFF BIN AZAHARNo ratings yet
- Ikea - Porter Five Force AnalysisDocument8 pagesIkea - Porter Five Force AnalysisAnuj KaulNo ratings yet
- MNO Chapter 05 - Planning - The Foundation of Successful ManagementDocument13 pagesMNO Chapter 05 - Planning - The Foundation of Successful ManagementDouglas FongNo ratings yet
- 10 W9 OSH II Safety EthicsDocument8 pages10 W9 OSH II Safety EthicsZulKhaliliNo ratings yet
- Performance Appraisal Quality of WorkDocument6 pagesPerformance Appraisal Quality of WorkDolly Ramie100% (1)
- Industrial Relation Means The Relationship Between Employers and Employees in Course of Employment in Industrial Organ Is at IonsDocument3 pagesIndustrial Relation Means The Relationship Between Employers and Employees in Course of Employment in Industrial Organ Is at Ionsdeep_archeshNo ratings yet
- Name: Awais Farooq Roll No.: 28 Course: Introduction To Business Teacher: Prof. Fida Hussain Bukhari Topic: CSRDocument12 pagesName: Awais Farooq Roll No.: 28 Course: Introduction To Business Teacher: Prof. Fida Hussain Bukhari Topic: CSRroyawaisNo ratings yet
- The PROCESS OF WAGE DETERMINATIONDocument13 pagesThe PROCESS OF WAGE DETERMINATIONDaniel Peter100% (1)
- Perceived Organizational SupportDocument7 pagesPerceived Organizational SupportMuqaddas IsrarNo ratings yet
- Chapter 1-Introduction To OM-OPM530Document6 pagesChapter 1-Introduction To OM-OPM530Haikal MohamadNo ratings yet
- Globalisation and IrrDocument96 pagesGlobalisation and IrrVivek YadavNo ratings yet
- Chapter 3 Opm538Document4 pagesChapter 3 Opm538Yuyu ComelNo ratings yet
- MPOBDocument251 pagesMPOBjigyasamiddhaNo ratings yet
- The Manufacturing Sector in Malaysia PDFDocument17 pagesThe Manufacturing Sector in Malaysia PDFNazirah Abdul RohmanNo ratings yet
- Answer Template - Ads 460Document13 pagesAnswer Template - Ads 460Khairi 0181No ratings yet
- 5 Time Management Skills RelationshipDocument6 pages5 Time Management Skills Relationshipjamesdj88914No ratings yet
- Research ProposalDocument3 pagesResearch ProposalBenny JohnNo ratings yet
- Unemployment of Fresh Graduate in MalaysiaDocument2 pagesUnemployment of Fresh Graduate in MalaysiaxxyuhooxxNo ratings yet
- Etika KerjaDocument10 pagesEtika Kerjazzz1403No ratings yet
- Asm453 2Document10 pagesAsm453 2Megan Sikajat100% (1)
- Adopter CategoriesDocument6 pagesAdopter CategoriesCaroline Mputhia100% (1)
- Toward A Balanced Scorecard For Higher Education: Rethinking The College and University Excellence Indicators FrameworkDocument10 pagesToward A Balanced Scorecard For Higher Education: Rethinking The College and University Excellence Indicators FrameworkAmu CuysNo ratings yet
- Termination of Employment Under The Laws of Tanzania 1 PDFDocument9 pagesTermination of Employment Under The Laws of Tanzania 1 PDFsarfNo ratings yet
- Jurnal Kepimpinan PendidikanDocument19 pagesJurnal Kepimpinan PendidikanSj KrishnanNo ratings yet
- A Study On Employee PerceptionDocument4 pagesA Study On Employee PerceptionBalaji GajendranNo ratings yet
- Management by Objectives PDFDocument25 pagesManagement by Objectives PDFARslan AzizNo ratings yet
- Paetecs Values Lead To A Satisfied and Committed Workforce Founded in 1998 PaetecDocument3 pagesPaetecs Values Lead To A Satisfied and Committed Workforce Founded in 1998 PaetecDoreenNo ratings yet
- Organizational Well Being A New Theoretical Model and Recommendations For Future ResearchDocument22 pagesOrganizational Well Being A New Theoretical Model and Recommendations For Future ResearchJeeta SarkarNo ratings yet
- Peter WesterholmDocument17 pagesPeter WesterholmTuam SiNo ratings yet
- Fit For Work Good Practice SharingDocument12 pagesFit For Work Good Practice SharingFit for Work EuropeNo ratings yet
- Early Intervention - DR Juan Angel Jover - Chronic Conditions Summit 2014Document10 pagesEarly Intervention - DR Juan Angel Jover - Chronic Conditions Summit 2014Fit for Work EuropeNo ratings yet
- FFW 2012 Summit - WernerDocument10 pagesFFW 2012 Summit - WernerFit for Work EuropeNo ratings yet
- Prof Stephen Bevan - Fit For Work Europe Summit 2013 PDFDocument9 pagesProf Stephen Bevan - Fit For Work Europe Summit 2013 PDFFit for Work EuropeNo ratings yet
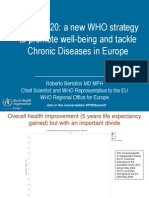
- Health2020: A New WHO Strategy To Promote Well-Being and Tackle Chronic Diseases in EuropeDocument16 pagesHealth2020: A New WHO Strategy To Promote Well-Being and Tackle Chronic Diseases in EuropeFit for Work EuropeNo ratings yet
- FFW 2012 Summit - FBKDocument12 pagesFFW 2012 Summit - FBKFit for Work EuropeNo ratings yet
- N Caeyers and S SmithDocument8 pagesN Caeyers and S SmithFit for Work EuropeNo ratings yet
- B DanuserDocument6 pagesB DanuserFit for Work EuropeNo ratings yet
- MSD Initiatives in DenmarkDocument3 pagesMSD Initiatives in DenmarkFit for Work EuropeNo ratings yet
- FFW Bulletin #1 April 2012Document3 pagesFFW Bulletin #1 April 2012Fit for Work EuropeNo ratings yet
- Chronic Conditions: The Importance of National and Regional Planning For The Management of MsdsDocument11 pagesChronic Conditions: The Importance of National and Regional Planning For The Management of MsdsFit for Work EuropeNo ratings yet
- Welcome Address by Steve BevanDocument9 pagesWelcome Address by Steve BevanFit for Work Europe100% (1)
- Morning Session - Reportback From Delegate WorkshopsDocument6 pagesMorning Session - Reportback From Delegate WorkshopsFit for Work EuropeNo ratings yet
- EU FFW 2011 Press Release FINALDocument2 pagesEU FFW 2011 Press Release FINALFit for Work EuropeNo ratings yet
- EU FFW 2011 Coalition BackgrounderDocument3 pagesEU FFW 2011 Coalition BackgrounderFit for Work EuropeNo ratings yet
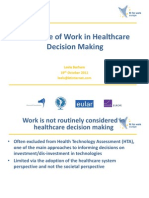
- The Place of Work in Healthcare Decision MakingDocument6 pagesThe Place of Work in Healthcare Decision MakingFit for Work EuropeNo ratings yet
- EU FFW 2011 MSD BackgrounderDocument3 pagesEU FFW 2011 MSD BackgrounderFit for Work EuropeNo ratings yet
- WBSEDCL OE AdmitDocument1 pageWBSEDCL OE AdmitSid SenguptaNo ratings yet
- Language Learning - CALLA - Cognitive Academic Language Learning Approach (CALLA)Document2 pagesLanguage Learning - CALLA - Cognitive Academic Language Learning Approach (CALLA)marie geronaNo ratings yet
- Canon 1-10 With Cases (Legal Ethics)Document45 pagesCanon 1-10 With Cases (Legal Ethics)Maria Resper100% (1)
- Roache Six C of CaringDocument3 pagesRoache Six C of CaringTutorshub Assignmenthelp PlatformNo ratings yet
- Aalto Et Al Eds - International Studies, Interdisciplinary ApproachesDocument293 pagesAalto Et Al Eds - International Studies, Interdisciplinary ApproachesSteffan Wyn-JonesNo ratings yet
- Five Conversations FrameworkDocument4 pagesFive Conversations FrameworkscorpionrockNo ratings yet
- Mapeh-6 Q4 W6-DLLDocument4 pagesMapeh-6 Q4 W6-DLLArlene Durban100% (2)
- MCS 034 PDFDocument3 pagesMCS 034 PDFRajat KoundalNo ratings yet
- Preservation Dallas Briefing To Dallas City CouncilDocument28 pagesPreservation Dallas Briefing To Dallas City CouncilRobert WilonskyNo ratings yet
- Supplier Security Assessment QuestionnaireDocument9 pagesSupplier Security Assessment QuestionnaireAhmed M. SOUISSI100% (1)
- Milk Tea Industry: An Exploratory Study: February 2020Document9 pagesMilk Tea Industry: An Exploratory Study: February 2020NING ANGELNo ratings yet
- Knewton Adaptive Learning WhitepaperDocument15 pagesKnewton Adaptive Learning WhitepaperWagane FayeNo ratings yet
- Teadrop Milk Tea ShopDocument36 pagesTeadrop Milk Tea ShopAlelei BungalanNo ratings yet
- Faqs On Foreign Investment in The PhilippinesDocument8 pagesFaqs On Foreign Investment in The PhilippinesVanillaSkyIIINo ratings yet
- Elsevier Journal FinderDocument4 pagesElsevier Journal FinderLuminita PopaNo ratings yet
- Child Abuse and Security Challenges in NigeriaDocument6 pagesChild Abuse and Security Challenges in NigeriaEditor IJTSRDNo ratings yet
- PresDraft 1Document38 pagesPresDraft 1Pradipta RohimoneNo ratings yet
- Ecocentrism: April 2019Document7 pagesEcocentrism: April 2019Shivam TiwariNo ratings yet
- SEAMEODocument279 pagesSEAMEOEdith PasokNo ratings yet
- AdddadadDocument3 pagesAdddadadZahra Alexä DavidsonNo ratings yet
- The Occult Character of The United NationsDocument10 pagesThe Occult Character of The United NationsLee T MatsNo ratings yet
- Ramirez, Kamille Alein M. - Komunikasyon W8Document2 pagesRamirez, Kamille Alein M. - Komunikasyon W8TcherKamilaNo ratings yet
- People V DoriaDocument2 pagesPeople V DoriaKhemshelly Titular FandialanNo ratings yet
- MakerBot in The Classroom PDFDocument146 pagesMakerBot in The Classroom PDFkreatosNo ratings yet
- Swot Analysis Open UniversityDocument36 pagesSwot Analysis Open UniversityIssa ChavezNo ratings yet
- Business Writing Quick ReferenceDocument3 pagesBusiness Writing Quick ReferencesbahourNo ratings yet
- ObhrmDocument30 pagesObhrmvamaNo ratings yet
- Semi-Detailed Lesson Plan in Teaching Mathematics Grade 9Document3 pagesSemi-Detailed Lesson Plan in Teaching Mathematics Grade 9ERIX VALMADRIDNo ratings yet
- Creative Strategy: Implementation and EvaluationDocument61 pagesCreative Strategy: Implementation and EvaluationGraphic GeniusNo ratings yet
- M-38 Stern Tube SealsDocument246 pagesM-38 Stern Tube SealsMehmet AGAGÜNDÜZNo ratings yet