LOOPOGRAM
Richard Danieli
�Patient Information
A 68 year old male with history of muscle
invading bladder cancer.
Post operative robotic assisted radical
cystoprostatectomy
Post operative ileal conduit urinary
diversion performed
�Patient History
History of bladder cancer
Prior CT
Filling defects in the dilated left renal pelvis
Absence of contrast opacification of the left
ureter,
Recommend direct inspection of the left
collecting system with cystoscopy and
ureteroscopy.
Interval worsening of the left
hydroureteronephrosis.
Anastomotic stricture at the junction between
the ureter and ileal conduit cannot be
excluded
�Reason for the
Examination
Recommendation from prior CT
Evaluate Ileal Conduit
Evaluate left ureter by retrograde
contrast administration
�Relevant Information
History of bladder cancer
Obstructed proximal left ureter seen on
prior CT
�Radiographic Procedure
24-gauge Foley catheter inserted into stoma
with 30 cc balloon inflated
Conray-60 introduced into ileal conduit by
gravity infusion
Reflux into right ureter
No contrast entered the left ureter despite
various positional changes and delayed
imaging.
Patient vomited possibly due to relative over
distention of the ileal bladder in attempts to
induce left ureteral reflux
�Examination Results
Normal right upper urinary tract
Normal ileal conduit contour
No reflux into left ureter due to
obstruction at the ureteroileal junction
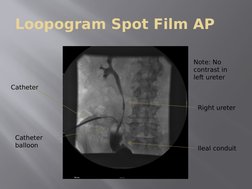
�Loopogram Spot Film AP
Note: No
contrast in
left ureter
Catheter
Right ureter
Catheter
balloon
Ileal conduit
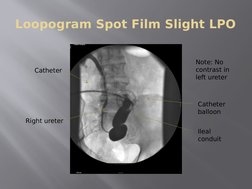
�Loopogram Spot Film Slight LPO
Catheter
Note: No
contrast in
left ureter
Catheter
balloon
Right ureter
Ileal
conduit
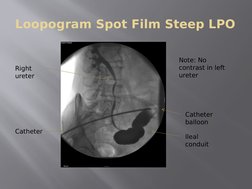
�Loopogram Spot Film Steep LPO
Right
ureter
Note: No
contrast in left
ureter
Catheter
balloon
Catheter
Ileal
conduit
�Abdomen/Pelvis CT with IV
Contrast Coronal Image
IV contrast
in right
ureter
IV contrast
remained in
left renal
pelvis
�Abdomen/Pelvis CT with IV
Contrast Axial Image
IV
contrast
in right
ureter
IV contrast
remained
in left renal
pelvis
�Differential Diagnosis
No contrast extravasated therefore obstructed
Ureteral obstruction post ileal conduit
Improperly fashioned anastomosis
Ischemia of the ureter with subsequent fibrosis and
stricture
Recurrent tumor in the ureter (rare)
Infection or abscess formation with reaction
Edema
Calculus
Sloughed papilla
Adhesions or scarring.
Torsion or compression at the sigmoid
�Discussion
No extravasation of contrast outside of
the ileal conduit or the right ureter
Normal contour of ileal conduit and right
ureter
No contrast filling into the left ureter
during the loopogram.
Left ureter not evaluated from retrograde
contrast administration via loopogram or
antegrade contrast administration via CT
�Suggestions
Renal ultrasound
Renal radionuclide studies,
Percutaneous nephrogram/ureterogram
Intravenous pyelogram (IVP)
Abdomen/pelvis CT (with oral contrast,
with and without IV contrast)
�Discussion Questions
John:
1. Where are post operative ileal conduit obstructions
most common?
2. Besides obstruction, what is the other most common
abnormality post operative ileal conduit surgery.
Stacy:
1. Describe pseudoobstruction (conduit malfunction) and
the cause.
2. What is a mucus plug in reference to a loopogram?
Tina:
1. Describe two renal complications of an ileal conduit.
2. What risks are associated with an excessive length of
an ileal conduit?
�References
Appleby,S.,&Atala,A.(2010,September2).UrostomyandContinentUrinaryDiversion.National
Kidney and Urologic Diseases Information Clearinghouse.RetrievedJuly7,2012,from
http://kidney.niddk.nih.gov/kudiseases/pubs/urostomy/index.aspx
Banner,M.P.,Pollack,H.M.,Bonavita,J.A.,&Ellis,P.S.(1984).Theradiologyofurinary
diversions.Radiographics,4,885-913.Retrievedfrom
http://radiographics.rsna.org/content/4/6/885.full.pdf+html?sid=b58c27e0-59a3-40e3-bba6-39316da2f
87d
Fernbach,S.,&Holland,E.(1988).Undiversionoftheurinarytract:Thepre-andpostoperatie
evaluation.Radiographics,8,213-233.Retrievedfrom
http://radiographics.rsna.org/content/8/2/213.full.pdf+html?sid=b58c27e0-59a3-40e3-bba6-39316da2f
87d
Noble,J.,Amin,Z.,Kessel,D.,&Rickards,D.(1994).Recurrentuppertracturothelialtumours:the
useofloopographyfollowingcystectomyforbladdercancer.British Journal of Radiology,67(803),
1057-1061.Retrievedfromhttp://www.ncbi.nlm.nih.gov/pubmed/7820396
Thiruchelvam,N.,Harrison,M.,&Page,A.C.(2007).Thedoublewiretechnique:animproved
methodfortreatingchallendingureteroilealanastomoticstricturesandocclusions.British Journal of
Radiology,80,103-106.Retrievedfromhttp://bjr.birjournals.org/content/80/950/103.long