MECHANISM OF
MUSCLE
CONTRACTION
Ginus Partadiredja
The Department of Physiology
UGM, Yogyakarta
� Muscle = neuron excited chemically, electrically,
mechanically to produce action potentials
Muscle neuron contractile mechanism activated by
action potentials
�Skeletal muscle:
cross-striations
does not contract without innervation
lacks anatomic & functional connections between fibers
voluntary control
Cardiac muscle:
cross-striations
functionally syncytial
contracts rhythmically in the absence of external innervation
contains pacemaker
Smooth muscle:
Lacks cross-striations
functionally syncytial
contains pacemaker
� Skeletal muscle muscle fibers myofibrils
Muscle fiber: multinucleated, long, cylindrical, single cell
surrounded by sarcolemma (cell membrane)
� Skeletal muscle muscle fibers myofibrils filaments
�Hexagonal pattern
� Filaments = contractile proteins:
Myosin II (thick filament)
Actin
Tropomyosin
Troponin: - Troponin I
thin filament
- Troponin T
- Troponin C
�Thick filaments A bands
Thin filaments I bands
�� Myosin 2 globular heads & long tail
Head of myosin contains actin-binding site & catalytic site
that hydrolize ATP
� Thin filaments two chains of actin
Tropomyosin in the groove of actin
Troponin: T binds other troponin to tropomyosin
I inhibits the interaction of myosin & actin
C contains the binding sites for Ca+2
� Sarcotubular system = T system + sarcoplasmic reticulum
T system of tubules + adjacent terminal cisternae = triad
T system rapid transmission of action potentials from
the cell membrane to the fibrils
� The resting membrane potential of muscle = -90 mV
The action potential = 2 4 ms
The speed along the muscle = 5 m/s
The absolute refractory period = 1 3 ms
The distribution of ions nerve cells
Depolarization = Na+ influx
Repolarization = K+ efflux
Depolarization starts at motor end plate transmitted
along the fiber contractile response
�Sequence of events during transmission from the motor
nerve the muscles = transmission in synapses between
neurons
�Sequence of Events in Contraction and Relaxation of
Skeletal Muscle
Steps in Contraction:
1. Discharge of motor neuron end of motor neuron Ca+2
enters the endings
�2. Release of transmitter (acetylcholine) at motor end-plate
3. Binding of acetylcholine to nicotinic acetylcholine
receptors (concentrated at the tops of the junctional folds)
�Junctional folds
�4. Increased Na+ and K+ conductance in end-plate membrane
5. Generation of end-plate potential
6. Generation of action potential in muscle fibers
�7. Inward spread of depolarization along T tubules
excitation contraction coupling
8. Release of Ca+2 from terminal cisterns of sarcoplasmic
reticulum and diffusion to thick and thin filaments
�9. Binding of Ca+2 to troponin C, uncovering myosin-binding
sites on actin (at resting, troponin I is tightly bound to actin
and tropomyosin covers the sites where myosin heads bind
to actin)
ATP is then split ADP + Pi contraction
�10. Formation of cross-linkages between actin and myosin
and sliding of thin on thick filaments, producing movement
���Steps in Relaxation:
1. Ca+2 pumped back into sarcoplasmic reticulum
diffuses into the terminal cisterns, ready to be released
by next action potential
2. Release of Ca+2 from troponin
3. Cessation of interaction between actin and myosin
�Muscular Contraction
The width of A bands is constant
Z lines move closer
��Production of ATP in Muscle Fibers (Tortora & Derrickson,
2006)
3 ways of ATP production:
1. From creatine phosphate
2. Anaerobic cellular respiration (ATP-producing reactions
not requiring oxygen)
3. Aerobic cellular respiration (ATP-producing reactions
requiring oxygen, in mitochondria)
�1. Creatine Phosphate
Creatine: small amino acid-like molecule formed in liver,
kidneys, pancreas transported to muscles
Relaxed muscles creatine phosphate 3-4x > ATP
Relaxation: ATP + creatine creatine phosphate + ADP
(by creatine kinase)
Contraction: creatine phosphate + ADP ATP + creatine
(by creatine kinase)
For 15 seconds contraction (100-m dash)
�2. Anaerobic Cellular Respiration
Creatine phosphate is depleted then:
Glucose (from blood or from the breakdown of glycogen in
muscles) glycolysis 2 pyruvic acid + 2 ATP (produces
4 ATP but net gain of 2 ATP)
Pyruvic acid mitochondria, aerobic respiration ATP
No oxygen (anaerobic) in cytosol: 80% Pyruvic acid
lactic acid blood (becomes acid) liver convert back
into glucose
For 30 - 40 seconds activity (400-m race)
�3. Aerobic Cellular Respiration
Sources of ATP: pyruvic acid, fatty acid (breakdown of
triglycerides; yields > 100 ATP), amino acids (breakdown
of proteins)
Sufficient oxygen: Pyruvic acid mitochondria
oxydized ATP + CO2 + H2O + heat
Slower than glycolysis, but yields 36 ATP
Sources of oxygen: hemoglobin & myoglobin
For > 10 minutes activity (marathon race)
�Energy Sources (Ganong, 2005)
ATP + H2O ADP + H3PO4 + 7.3 kcal
Phosphorylcreatine + ADP Creatine + ATP
Rest & light exercise:
FFA CO2 + H2O + ATP
Increased intensity of exercise
Glucose + 2 ATP (or glycogen + 1 ATP) 2 Lactic acid + 4 ATP
(anaerobic)
Glucose + 2 ATP (or glycogen + 1 ATP) 6CO2 + 6H2O + 40ATP
(aerobic)
� 100-m dash (10 seconds) 85% of energy is derived
anaerobically
2-mile race (10 minutes) 20% of energy is derived
anaerobically
long-distance race (60 minutes) 5% of energy is derived
anaerobically
� Muscle fatigue: The inability of muscle to maintain force
of contraction after prolonged activity, caused by:
Inadequate release of Ca+2 from sarcoplasmic
reticulum
Depletion of creatine phosphate
ATP levels = resting levels
Insufficient oxygen
Depletion of glycogen
Buildup of lactic acid & ADP
Failure of action potentials in releasing ACh
�Oxygen Consumption after Exercise
Oxygen debt added oxygen, over and above the
resting oxygen consumption, taken into the body after
exercise
1. Convert lactic acid glycogen stores in liver (small
amount)
2. Resynthesize creatine phosphate & ATP
3. Replace the oxygen removed from myoglobin
Much of lactic acid pyruvic acid for ATP production
(heart, liver, kidneys, skeletal muscles)
Better term: recovery oxygen uptake (
chemical
reactions, heart & muscles still working, recovery
processes)
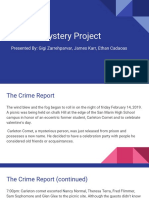
�Types of Contraction
Isotonic (A) and isometric (B) contraction
�Types of Contraction
Isometric (same length) contraction: Contraction occurs
without an appreciable decrease in the length of the whole
muscle do not work (work = force x distance)
� Isotonic (same tension) contraction: Contraction against
a constant load do work
�Isotonic contraction
Cause more damage
�Muscle twitch: brief contraction followed by relaxation of all
muscle fibers in a motor unit caused by a single action
potential in its motor neuron
Fast muscle fibers: fine movements (7.5 ms)
Slow muscle fibers: gross movements (100 ms)
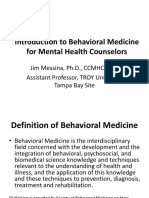
�Summation of Contractions
No refractory period such as in neurons in muscle fibers
Repeated stimulation summation of contractions
Tetanus (tetanic contraction) continuous contraction:
Fused (complete) tetanus
Unfused (incomplete) tetanus
��Types of Muscle Fibers
Type I
Other names
Slow, oxidative,
red muscles
Type II
Fast;
glycolytic;
white muscles
Myosin isoenzyme ATPase rate Slow
Fast
Ca+2 pumping capacity of
sarcoplasmic reticulum
Moderate
High
Diameter
Moderate
Large
Glycolytic capacity
Moderate
High
Oxidative capacity (content of
mitochondria, capillary
density, myoglobin content)
High
Low
Examples
Long muscles of
the back
Estraocular
�Charateristics
Functions
Examples
Type I
(Red muscles)
Slow response;
long latency;
adapted for
long, slow
contractions
Type II
(White muscles)
Short twitch
durations
Posture
maintenance
Long muscles in
the back
Fine, skilled
movements
Extraocular
muscles, hand
muscles
�Slow
Oxidative
Fibers
Fast
OxidativeGlycolytic
Fibers
Fast
Glycolytic
Fibers
Fiber
diameter
Myoglobin
content
Mitochondria
Smallest
Intermediate
Largest
Large
amount
Many
Large
amount
Many
Small
amount
Few
Capillaries
Color
Many
Red
Many
Red-pink
Few
White
(pale)
Structural
Characteristi
c
�Slow
Oxidative
Fibers
Fast
OxidativeGlycolytic
Fibers
Fast
Glycolytic
Fibers
Capacity of
generating
ATP
High;
aerobic
respiration
Intermediate; Low;
aerobic &
anaerobic
anaerobic
(glycolysis)
(glycolysis)
Rate of ATP
hydrolysis
Contraction
velocity
Fatigue
Slow
Fast
Fast
Slow
Fast
Fast
High
Intermediate
Low
Functional
Characteristi
c
�Slow
Oxidative
Fibers
Fast
OxidativeGlycolytic
Fibers
Fast
Glycolytic
Fibers
Creatine
kinase
Lowest
amount
Intermediate
amount
Highest
amount
Glycogen
stores
Low
Intermediate
High
Order of
recruitment
First
Second
Third
Location
Postural
muscles
(e.g. neck)
Lower limb
Upper limb
�Slow
Oxidative
Fibers
Primary Maintaining
function posture;
s
aerobic
endurance
(running a
marathon)
Fast
OxidativeGlycolytic
Fibers
Fast Glycolytic
Fibers
Walking,
sprinting
Rapid, intense
movement of
short duration
(weight lifting;
throwing a ball)
�Disorders and Abnormalities
Myasthenia gravis: skeletal muscles are weak and tire
easily; caused by autoantibodies destroying nicotinic
acetylcholine receptors
Lambert-Eaton syndrome: muscle weakness; caused by
antibodies against Ca+2 channels in the nerve endings
Denervation hypersensitivity
Contracture: No relaxation due to the inhibition of Ca+2
transport into the reticulum
�Disorders and Abnormalities
Hypotonia: decreased or lost muscle tone
Flaccid paralysis loss of muscle tone, loss/ reduction
of tendon reflexes, atrophy, degeneration of muscles
(disorders of nervous system; electrolytes imbalances
(Na+, Ca+2, Mg+2)
Hypertonia: increased muscle tone
Spastic paralysis increased muscle tone, tendon
reflexes, pathological reflexes (Babinski sign)
Rigidity increased muscle tone, not reflexes
(tetanus)
�Disorders and Abnormalities
Muscular dystrophy: progressive weakness of skeletal
muscle caused by mutations in genes for muscle proteins
Duchenes muscular dystrophy dystrophin protein is
absent from muscle; X-linked; fatal by 30 y/o
Metabolic myopathies (e.g. McArdles syndrome)
mutations in genes of enzymes involved in carbohydrates,
fats, and proteins, metabolism
Myotonia muscle relaxation is prolonged after
contraction; abnormal genes in chromosomes 7, 17, or 19,
which produce abnormalities of Na+ or Cl- channels
�References
1. Ganong WF (2005). Review of Medical Physiology, 22nd
ed. Chapter 3, Pages: 65-78; Chapter 4, Pages: 116-120
2. Tortora GJ & Derrickson B (2006). Principles of Anatomy
and Physiology, 11th ed. Chapter 10, Pages: 290-314.