You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pathophysiology AML DiagramDocument4 pagesPathophysiology AML DiagramKlerra Hope60% (5)
- Moore's Clinically Oriented Anatomy 6th EdDocument4 pagesMoore's Clinically Oriented Anatomy 6th EdJohna Pauline Mandac67% (6)
- Pathology Outlines - Papillary Carcinoma - GeneralDocument6 pagesPathology Outlines - Papillary Carcinoma - Generalpatka1rNo ratings yet
- Digestive SystemDocument48 pagesDigestive SystemJerilee SoCute WattsNo ratings yet
- The Circulatory System-: TransportDocument13 pagesThe Circulatory System-: TransportJerilee SoCute WattsNo ratings yet
- The Digestive System: Cont'd (From Swallowing)Document56 pagesThe Digestive System: Cont'd (From Swallowing)Jerilee SoCute WattsNo ratings yet
- The HeartDocument42 pagesThe HeartJerilee SoCute WattsNo ratings yet
- The Digestive System EssayDocument3 pagesThe Digestive System EssayJerilee SoCute Watts0% (1)
- Reproduction and DevelopmentDocument53 pagesReproduction and DevelopmentJerilee SoCute WattsNo ratings yet
- Review Questions - HeartDocument1 pageReview Questions - HeartJerilee SoCute WattsNo ratings yet
- Lecture 2 Cardiovascular SystemDocument70 pagesLecture 2 Cardiovascular SystemJerilee SoCute WattsNo ratings yet
- Lecture 1 Cardiovascular SystemDocument70 pagesLecture 1 Cardiovascular SystemJerilee SoCute WattsNo ratings yet
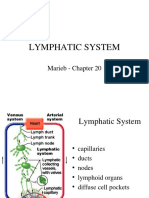
- Lymphatic System: Marieb Chapter 20Document22 pagesLymphatic System: Marieb Chapter 20Jerilee SoCute WattsNo ratings yet
- Endocrine System: Glands & HormonesDocument78 pagesEndocrine System: Glands & HormonesJerilee SoCute WattsNo ratings yet
- Respiratory Centers of The BrainDocument36 pagesRespiratory Centers of The BrainJerilee SoCute WattsNo ratings yet
- Past Papers Section2Document13 pagesPast Papers Section2Jerilee SoCute Watts50% (2)
- Endocrine System: Hormones & HomeostasisDocument32 pagesEndocrine System: Hormones & HomeostasisJerilee SoCute WattsNo ratings yet
- The Integumentary System: Human Anatomy, 3rd Edition Prentice Hall, © 2001Document43 pagesThe Integumentary System: Human Anatomy, 3rd Edition Prentice Hall, © 2001Jerilee SoCute WattsNo ratings yet
- Gametogenesis: - Gametes Develop in The Gonads (Sex Cells)Document12 pagesGametogenesis: - Gametes Develop in The Gonads (Sex Cells)Jerilee SoCute WattsNo ratings yet
- Endocrine System DisordersDocument83 pagesEndocrine System DisordersJerilee SoCute Watts0% (1)
- The Female Reproductive System: by Justine Wilson and Kim IwanskiDocument18 pagesThe Female Reproductive System: by Justine Wilson and Kim IwanskiJerilee SoCute WattsNo ratings yet
- Cysts of The JawsDocument75 pagesCysts of The JawsSwetha KaripineniNo ratings yet
- Anatomy and Physiology of Male Reproductive SystemDocument8 pagesAnatomy and Physiology of Male Reproductive SystemAdor AbuanNo ratings yet
- The Plant and Animal CellsDocument2 pagesThe Plant and Animal CellsLeny MacraNo ratings yet
- Carrier-Mediated Dermal DeliveryDocument587 pagesCarrier-Mediated Dermal DeliveryVanderval SIlva de OliveiraNo ratings yet
- Q2 Summative Test 1ST CYCLEDocument11 pagesQ2 Summative Test 1ST CYCLEJanessa EnteaNo ratings yet
- Circulatory SystemDocument31 pagesCirculatory SystemGeonardo100% (3)
- 14-16 Juli 2022, Jayapura I Post Test (Jawaban)Document10 pages14-16 Juli 2022, Jayapura I Post Test (Jawaban)Abdul Charis KonorasNo ratings yet
- AUBF - Amniotic Fluid and Semen Study MaterialDocument10 pagesAUBF - Amniotic Fluid and Semen Study MaterialVienna Jamaica Be Cari-CariNo ratings yet
- Frizzell 2005Document20 pagesFrizzell 2005GiorgianaNo ratings yet
- Rosemary Estrada - Histology Lab NotebookDocument12 pagesRosemary Estrada - Histology Lab NotebookRosemary EstradaNo ratings yet
- Hematology Reference RangeDocument1 pageHematology Reference RangeNheeya WarzNo ratings yet
- DoReMi Ni Lalala EDITED PDFDocument156 pagesDoReMi Ni Lalala EDITED PDFEleonor Katreeya LimsiNo ratings yet
- What To Study Nervous Endocrine ReproDocument2 pagesWhat To Study Nervous Endocrine ReproSean CampbellNo ratings yet
- Komunikasi Antar Sel: Irma Yuniar Wardhani, M.PDDocument12 pagesKomunikasi Antar Sel: Irma Yuniar Wardhani, M.PDIrma YuniarNo ratings yet
- Autonomic Nervous System - Anatomy - LecturioDocument20 pagesAutonomic Nervous System - Anatomy - LecturioAlfred ZhikNo ratings yet
- Maternal Physiology During PregnancyDocument28 pagesMaternal Physiology During PregnancyPutra MahautamaNo ratings yet
- The Theater of Anatomy - The Anatomical Preparations of Honore Fragonard PDFDocument18 pagesThe Theater of Anatomy - The Anatomical Preparations of Honore Fragonard PDFFrancisco SantosNo ratings yet
- All in Golden Kool Medic PDFDocument570 pagesAll in Golden Kool Medic PDFDrFaryal AbbassiNo ratings yet
- Williams Obstertics, Twenty-Second Edition - Page 619 630Document57 pagesWilliams Obstertics, Twenty-Second Edition - Page 619 630Bharat ThapaNo ratings yet
- Melanoma MalignaDocument28 pagesMelanoma MalignaDila Muflikhy PutriNo ratings yet
- Study of Plant Cells in Hypertonic Solution: Experiment: PlasmolysisDocument2 pagesStudy of Plant Cells in Hypertonic Solution: Experiment: PlasmolysisJyoti DahiyaNo ratings yet
- AP Psych 2.3 Notes - Nervous and Endocrine SystemDocument2 pagesAP Psych 2.3 Notes - Nervous and Endocrine SystemIan BurtNo ratings yet
- A Care Study On Normal Spontaneous Vaginal Delivery Submitted To: Ms. Maria Lowela V. ElopreDocument8 pagesA Care Study On Normal Spontaneous Vaginal Delivery Submitted To: Ms. Maria Lowela V. ElopreJhoi CastroNo ratings yet
- CELL-THE UNIT OF LIFE-Ribosomes, CytoskeletonDocument19 pagesCELL-THE UNIT OF LIFE-Ribosomes, CytoskeletonHridyanshu Singh RoyNo ratings yet
- Bab Skripsi Dan Dapus IpmDocument3 pagesBab Skripsi Dan Dapus IpmAnggi Anggraeni Ratu GumelarNo ratings yet
- Sistem Imun 2Document20 pagesSistem Imun 2CameliaMasrijalNo ratings yet
- MuscoDocument1 pageMuscoMarean NicholeNo ratings yet