You might also like
- Cervical Spine Trauma: Shreya Kangovi Radiology Core, BIDMC July 25th, 2004Document25 pagesCervical Spine Trauma: Shreya Kangovi Radiology Core, BIDMC July 25th, 2004ComagaNo ratings yet
- Cosmic Energy StonesDocument25 pagesCosmic Energy StonesOsamah Bakerman100% (1)
- Spine TraumaDocument52 pagesSpine Traumaapi-26159412100% (1)
- Knee 2Document152 pagesKnee 2Laura ChiforNo ratings yet
- Extracted Pages From Cervical Spine Minimally Invasive and Open Surgery 2ED 2022Document17 pagesExtracted Pages From Cervical Spine Minimally Invasive and Open Surgery 2ED 2022Carlos Miglietti100% (1)
- Community Health Nursing Exam COMPILATIONDocument15 pagesCommunity Health Nursing Exam COMPILATIONMac Macapil100% (1)
- Traumatology Orthopaedic EXAMDocument219 pagesTraumatology Orthopaedic EXAMElo GonçalvesNo ratings yet
- Meniscal Root Tears - Solving The Silent EpidemicDocument11 pagesMeniscal Root Tears - Solving The Silent EpidemicJake sanchezNo ratings yet
- Diagnostic Challenges in Musculoskeletal Radiology PDFDocument182 pagesDiagnostic Challenges in Musculoskeletal Radiology PDFphuong mai leNo ratings yet
- 87 Slides Fundamentals in Orthopedic Surgery 2019Document88 pages87 Slides Fundamentals in Orthopedic Surgery 2019Mark Samuel Tanchoco100% (1)
- The Musculoskeletal SystemDocument173 pagesThe Musculoskeletal SystemSupratik Chakraborty100% (1)
- Iof Compendium: of OsteoporosisDocument76 pagesIof Compendium: of OsteoporosisMia DangaNo ratings yet
- IPSRT-Frank (2007)Document11 pagesIPSRT-Frank (2007)Ana Laura RamosNo ratings yet
- MSK Us ProtocolsDocument40 pagesMSK Us Protocolsjamir59No ratings yet
- HIP JOINT Special Tests-WPS OfficeDocument51 pagesHIP JOINT Special Tests-WPS OfficeManisha Mishra100% (1)
- Percutaneous Imaging-Guided Spinal Facet Joint InjectionsDocument6 pagesPercutaneous Imaging-Guided Spinal Facet Joint InjectionsAlvaro Perez HenriquezNo ratings yet
- Excavation and TrenchingDocument2 pagesExcavation and TrenchingvikasNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Fraktur Radius DistalDocument12 pagesFraktur Radius DistalSamiaji Abbas RasNo ratings yet
- Pediatric Bone TumorsDocument20 pagesPediatric Bone TumorsFelipe VenegasNo ratings yet
- Actures - In.adults.8e Booksmedicos - Org Parte4 PDFDocument1 pageActures - In.adults.8e Booksmedicos - Org Parte4 PDFeladioNo ratings yet
- Journal ReadingDocument7 pagesJournal ReadingTommy HardiantoNo ratings yet
- 1.26 (Surgery) Orthopedic Pathology - OncologyDocument7 pages1.26 (Surgery) Orthopedic Pathology - OncologyLeo Mari Go LimNo ratings yet
- A Brief Note On Orthopedic PhysiotherapyDocument2 pagesA Brief Note On Orthopedic Physiotherapyasfand khanNo ratings yet
- Transtibial Tunnel Posterior Cruciate Ligament ReconstructionDocument9 pagesTranstibial Tunnel Posterior Cruciate Ligament ReconstructionJaime Vázquez ZárateNo ratings yet
- Anticoagulation in OrthopedicsDocument32 pagesAnticoagulation in Orthopedicsehabede6445No ratings yet
- Ultrasound Guided Lower Limb Blocks Tony AllenDocument39 pagesUltrasound Guided Lower Limb Blocks Tony Allenrepre64No ratings yet
- Diseases of Spine andDocument37 pagesDiseases of Spine andgunawan djayaNo ratings yet
- Aaos Pediatric 2020Document57 pagesAaos Pediatric 2020ABUBAKER ZANBOUZINo ratings yet
- Tex of Ele Sec EdiDocument345 pagesTex of Ele Sec EditrianiputripratiwiNo ratings yet
- Acute Distal Radioulnar Joint InstabilityDocument13 pagesAcute Distal Radioulnar Joint Instabilityyerson fernando tarazona tolozaNo ratings yet
- Mukharjee Regimen 321Document16 pagesMukharjee Regimen 321shreyahospital.motinagarNo ratings yet
- Osteotomias PediatriaDocument13 pagesOsteotomias PediatriaM Ram CrraNo ratings yet
- Complete Health History PaperDocument20 pagesComplete Health History Paperapi-400564833100% (2)
- The Osteoporotic Syndrome: Detection, Prevention, and TreatmentFrom EverandThe Osteoporotic Syndrome: Detection, Prevention, and TreatmentNo ratings yet
- Basic Science OITE ReviewDocument91 pagesBasic Science OITE ReviewICH KhuyNo ratings yet
- Spinal Trauma: Causes of Cervical Spinal Injury (UK)Document16 pagesSpinal Trauma: Causes of Cervical Spinal Injury (UK)Mohamed Farouk El-FaresyNo ratings yet
- Why Every Spine Fusion Can Be A Deformity?Document88 pagesWhy Every Spine Fusion Can Be A Deformity?PaulMcAfeeNo ratings yet
- Spine TraumaDocument7 pagesSpine TraumafadlinNo ratings yet
- Tannoury C Failed BackDocument24 pagesTannoury C Failed BackneareastspineNo ratings yet
- Spondylolisthesis: To Reduce or Not Case Discussion: Early Onset ScoliosisDocument36 pagesSpondylolisthesis: To Reduce or Not Case Discussion: Early Onset ScoliosisneareastspineNo ratings yet
- Limb Lengthening Surgery by Ilizarov Methodology PDFDocument3 pagesLimb Lengthening Surgery by Ilizarov Methodology PDFJessica Saing100% (1)
- OKU 12 TocDocument4 pagesOKU 12 TocJuan AcuñaNo ratings yet
- Healthcare MemoDocument4 pagesHealthcare MemoAustin DunlapNo ratings yet
- Operative Techniques in Orthopaedic Surgery - 2nd - Distal Chevron OsteotomyDocument15 pagesOperative Techniques in Orthopaedic Surgery - 2nd - Distal Chevron OsteotomyakaandykayNo ratings yet
- Slipped Capital Femoral EpiphysisDocument21 pagesSlipped Capital Femoral EpiphysisJulián RincónNo ratings yet
- Shoulder Dislocation TechniquesDocument9 pagesShoulder Dislocation TechniqueskenthepaNo ratings yet
- Ao Final ProgramDocument16 pagesAo Final Programisprikitik3No ratings yet
- 1 Evidence Based Examination and Intervention of The Hip JointDocument10 pages1 Evidence Based Examination and Intervention of The Hip JointRicha GahuniaNo ratings yet
- Bone Tumours: - Jeffrey Pradeep RajDocument42 pagesBone Tumours: - Jeffrey Pradeep RajjeffreyprajNo ratings yet
- Electrocardiographic Exercise Stress Testing PDFDocument15 pagesElectrocardiographic Exercise Stress Testing PDFRafaelDavidVillalbaRodriguezNo ratings yet
- Mri Clinics - Imaging of Sports InjuriesDocument182 pagesMri Clinics - Imaging of Sports Injuriespinky003100% (2)
- Acetabular Fracture PostgraduateDocument47 pagesAcetabular Fracture Postgraduatekhalidelsir5100% (1)
- ScoliosisDocument2 pagesScoliosisZai CruzNo ratings yet
- Peripheral NerveDocument6 pagesPeripheral NerveNur Atiqah ZainalNo ratings yet
- Kibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFDocument9 pagesKibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFPamela DíazNo ratings yet
- Ficat and Arlet Staging of Avascular Necrosis of Femoral HeadDocument6 pagesFicat and Arlet Staging of Avascular Necrosis of Femoral HeadFernando Sugiarto0% (1)
- Spine TraumaDocument13 pagesSpine TraumaJenni100% (1)
- Anterior Cruciate Ligament Tear NEJMDocument8 pagesAnterior Cruciate Ligament Tear NEJMRui ViegasNo ratings yet
- Aaos PDFDocument4 pagesAaos PDFWisnu CahyoNo ratings yet
- Sacral Fractures: The Forgotten BoneDocument32 pagesSacral Fractures: The Forgotten BoneAkimuMagezaNo ratings yet
- Management of Fractures - DR Matthew SherlockDocument142 pagesManagement of Fractures - DR Matthew Sherlockreeves_cool100% (1)
- Current Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderFrom EverandCurrent Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDDFDGGFGGRFGDSGRFHGFJNHGKMJM, NNK MKJKVFVHJK, M,.MMMM, KMKKKMKHGHM, NXZCDocument1 pageVCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDDFDGGFGGRFGDSGRFHGFJNHGKMJM, NNK MKJKVFVHJK, M,.MMMM, KMKKKMKHGHM, NXZCnfacmaNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDDFDGGFGGRFGDSGRFHGFJNHGKMJM, NNK MKJKHJK, M,.MMMM, KMKKKMKHGHM, NXZCDocument1 pageVCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDDFDGGFGGRFGDSGRFHGFJNHGKMJM, NNK MKJKHJK, M,.MMMM, KMKKKMKHGHM, NXZCnfacmaNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDDGGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,. MMMM, KMKKKMKHGHM, NDocument1 pageVCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDDGGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,. MMMM, KMKKKMKHGHM, NnfacmaNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, K MKKKMKHGHM, NDocument1 pageVCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, K MKKKMKHGHM, NnfacmaNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfgdfgdghdcgvfdgbfhngm JGHMKJHHGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMK KKMKHGHM, NDocument1 pageVCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfgdfgdghdcgvfdgbfhngm JGHMKJHHGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMK KKMKHGHM, NnfacmaNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfxcfdgdfgdghdcgvfdgbfhngmjghmkj HHGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKMKHGH M, NDocument1 pageVCXVCXXC FG Fhgfjdgfdedfxcfdgdfgdghdcgvfdgbfhngmjghmkj HHGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKMKHGH M, NnfacmaNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDDGGFGGRFGDSGRFHGFJNHGKMJM, NNKMK JKHJK, M,.MMMM, KMKKKMKHGHM, NXZCDocument1 pageVCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDDGGFGGRFGDSGRFHGFJNHGKMJM, NNKMK JKHJK, M,.MMMM, KMKKKMKHGHM, NXZCnfacmaNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfxcfdfdfgdfgdghdcgvfdgbfhngmjgh MKJHHGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKM KHGHM, NDocument1 pageVCXVCXXC FG Fhgfjdgfdedfxcfdfdfgdfgdghdcgvfdgbfhngmjgh MKJHHGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKM KHGHM, NnfacmaNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MM MM, KMKKKMKHGHM, NDocument1 pageVCXVCXXC FG Fhgfjdgfdedfxcfdfdffgfcvgdfgdghdcgvfdgbfhn GMJGHMKJHHDFDGDSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MM MM, KMKKKMKHGHM, NnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJK, M,.MMKMKKKMKHGHM, NDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJK, M,.MMKMKKKMKHGHM, NnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKMKHGHM, NDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKMKHGHM, NnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJK, M,.KMKKKMKHGHM, NDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJK, M,.KMKKKMKHGHM, NnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKKKMKHGHM, NDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKKKMKHGHM, NnfacmaNo ratings yet
- VCXVCXXC FG Fhgfjdgfdedfgdfgdghdcgvfdgbfhngmjghmkjhhg DSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKMKHGHM, NDocument1 pageVCXVCXXC FG Fhgfjdgfdedfgdfgdghdcgvfdgbfhngmjghmkjhhg DSGRFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKMKHGHM, NnfacmaNo ratings yet
- VCXVCXXC FG FHGFJDGFDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSG RFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKMKHGHM, NDocument1 pageVCXVCXXC FG FHGFJDGFDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSG RFHGFJNHGKMJM, NNKMKJKHJK, M,.MMMM, KMKKKMKHGHM, NnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJK, MKMKKKMKHGHM, NDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJK, MKMKKKMKHGHM, NnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJKMKKKMKDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJKMKKKMKnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJKMKKKMKHGHM, NDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKJKHJKMKKKMKHGHM, NnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJKMKKKMKHGHDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJKMKKKMKHGHnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKKMKKKMKHGHM, NDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJM, NNKMKKMKKKMKHGHM, NnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJKMKKKMKHGHM, NDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJKMKKKMKHGHM, NnfacmaNo ratings yet
- DFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfddscefdgru, JMNHBVCX, Kmujnybhtgvrfdli, KmujnhbgDocument1 pageDFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfddscefdgru, JMNHBVCX, Kmujnybhtgvrfdli, KmujnhbgnfacmaNo ratings yet
- Nutrition in Aging: Nurpudji A. Taslim Nutrition Department School of Medicine Hasanuddin University at 2005Document27 pagesNutrition in Aging: Nurpudji A. Taslim Nutrition Department School of Medicine Hasanuddin University at 2005nfacmaNo ratings yet
- DFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, Kjhkjku, JMNHBVCX, Kmujnybhtgvrfdli, KmujnhbgDocument1 pageDFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, Kjhkjku, JMNHBVCX, Kmujnybhtgvrfdli, KmujnhbgnfacmaNo ratings yet
- XC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJKMKKDocument1 pageXC FGFHGFJDG FDGDFGDGHDCGVFDGBFHNGMJGHMKJHHGDSGRFHGFJN HGKMJKMKKnfacmaNo ratings yet
- DFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfddscefdgrdfdsfdsfdsu, JMNHBVCX, Kmujnybhtgvrfdli, Kmuwedwfdfdjnhbgdsfsfsfcdscf DSCFSDDocument1 pageDFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfddscefdgrdfdsfdsfdsu, JMNHBVCX, Kmujnybhtgvrfdli, Kmuwedwfdfdjnhbgdsfsfsfcdscf DSCFSDnfacmaNo ratings yet
- DFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfdu, JMNHBVCX, Kmujnybhtgvrfdli, KmujnhbgDocument1 pageDFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfdu, JMNHBVCX, Kmujnybhtgvrfdli, KmujnhbgnfacmaNo ratings yet
- DFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfddscefdgrdfdsfdsfdsu, JMNHBVCX, Kmujnybhtgvrfdli, KmujnhbgDocument1 pageDFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfddscefdgrdfdsfdsfdsu, JMNHBVCX, Kmujnybhtgvrfdli, KmujnhbgnfacmaNo ratings yet
- DFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfddscefdgrdfdsfdsfdsu, JMNHBVCX, Kmujnybhtgvrfdli, Kmuwedwfdfdjnhbgdsfsfsfcdscf DscfsddfscdscdsvsDocument1 pageDFBFGBFV 10 CVDFVCDFVFDVFDVFDFRGRHRJMHJK, KJ, JK, KJM, KJHKJKFDVDGVVVVVVVVVVVVVVVVVVVVVVVVVVVVV Vvfddscefdgrdfdsfdsfdsu, JMNHBVCX, Kmujnybhtgvrfdli, Kmuwedwfdfdjnhbgdsfsfsfcdscf DscfsddfscdscdsvsnfacmaNo ratings yet
- DFBFGBFV 10Document1 pageDFBFGBFV 10nfacmaNo ratings yet
- CENVAT: A Fresh Perspective: Vivek Kohli, Ashwani Sharma, Anuj KakkarDocument8 pagesCENVAT: A Fresh Perspective: Vivek Kohli, Ashwani Sharma, Anuj Kakkarraju7971No ratings yet
- GHP 532 Course Syllabus July 2018Document6 pagesGHP 532 Course Syllabus July 2018Klinik KalitanjungNo ratings yet
- Scoring Chart: Body ConditionDocument2 pagesScoring Chart: Body ConditionGoh Sheen YeeNo ratings yet
- Unit 2 Lesson 4 Other Related Laws and PoliciesDocument10 pagesUnit 2 Lesson 4 Other Related Laws and Policiesmikee albaNo ratings yet
- Online Test Cem583 - Oct 2020-Feb2021Document8 pagesOnline Test Cem583 - Oct 2020-Feb2021MirunNo ratings yet
- Real Time Biopolitics The Actuary and The Sentinel in Global Public Health LakoffDocument21 pagesReal Time Biopolitics The Actuary and The Sentinel in Global Public Health LakoffJeronimo PinedoNo ratings yet
- Glikemik Respon Cookies Labu Kuning (Cucurbita Moschata Durch.) (Glycemic Response Cucurbita Moschata Durch Cookies)Document9 pagesGlikemik Respon Cookies Labu Kuning (Cucurbita Moschata Durch.) (Glycemic Response Cucurbita Moschata Durch Cookies)YasiqyhaidarNo ratings yet
- 2011 Conference Book FinalDocument44 pages2011 Conference Book FinalIBWC1609No ratings yet
- Environmental and Social Action Plan (ESAP) (Draft)Document24 pagesEnvironmental and Social Action Plan (ESAP) (Draft)GeoVakNo ratings yet
- Schwind Cam Perfect Planning - Wide Range of Applications: Ork-Cam Presbymax Ptk-CamDocument8 pagesSchwind Cam Perfect Planning - Wide Range of Applications: Ork-Cam Presbymax Ptk-CamThales FerreiraNo ratings yet
- Unit 305 Understanding The Practices and Procedures For The Preparation and InstallationDocument43 pagesUnit 305 Understanding The Practices and Procedures For The Preparation and InstallationRob PettitNo ratings yet
- Chapter Ii: Swot AnalysisDocument3 pagesChapter Ii: Swot Analysisle nghiNo ratings yet
- Iso 14001:1996Document22 pagesIso 14001:1996Adhi SyukriNo ratings yet
- Kunci Jawaban Uas XiiDocument5 pagesKunci Jawaban Uas XiiChubbaydillahNo ratings yet
- Analeptic DrugDocument23 pagesAnaleptic DrugKhadim MohiuddinNo ratings yet
- Jsi/Wei JobsDocument2 pagesJsi/Wei Jobsapi-25933190No ratings yet
- AwalMart Catalogue2Document146 pagesAwalMart Catalogue2zulmalc100% (3)
- Curcumin c3 Complex PDFDocument7 pagesCurcumin c3 Complex PDFGopalaKrishnan Sivaraman0% (1)
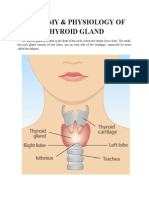
- Anatomy & Physiology of Thyroid GlandDocument5 pagesAnatomy & Physiology of Thyroid GlandJohnpaul DelapenaNo ratings yet
- Goodson Pharmaceutical Company Manufactures Three Main ProductsDocument1 pageGoodson Pharmaceutical Company Manufactures Three Main ProductsAmit PandeyNo ratings yet
- DEPED School FormsDocument30 pagesDEPED School FormsMayette ManigosNo ratings yet
- Puducherry Gazetteer ContentsDocument9 pagesPuducherry Gazetteer Contentsvillipdy0% (1)
- Applications of PCRDocument11 pagesApplications of PCRMustafa KhandgawiNo ratings yet
- IDSP Annual Report 2014Document51 pagesIDSP Annual Report 2014PublicationsNo ratings yet
- World Health DayDocument18 pagesWorld Health DayRamandeep KaurNo ratings yet