You might also like
- Wheat Belly by Dr. William DavisDocument9 pagesWheat Belly by Dr. William DavissimasNo ratings yet
- Daftar Tarif Untuk Eksternal 2020 PRODIADocument16 pagesDaftar Tarif Untuk Eksternal 2020 PRODIAKukuruyuk KukuruyukNo ratings yet
- CYANSmart App Sheets ENGDocument60 pagesCYANSmart App Sheets ENGMaria Alejandra Noguera Delgadillo100% (1)
- Co- and Post-Translational Modifications of Therapeutic Antibodies and ProteinsFrom EverandCo- and Post-Translational Modifications of Therapeutic Antibodies and ProteinsNo ratings yet
- Meconium Aspiration Syndrome: Walter Otieno Consultant PaediatricianDocument27 pagesMeconium Aspiration Syndrome: Walter Otieno Consultant PaediatricianMalueth AnguiNo ratings yet
- Obstetrics and GynaecologyDocument43 pagesObstetrics and Gynaecologylisserrano100% (1)
- Pediatric Reference Ranges Endocrinology 0981 PDFDocument14 pagesPediatric Reference Ranges Endocrinology 0981 PDFMMCSTORENo ratings yet
- Creatine Kinase: NAC. Kinetic UV. LiquidDocument2 pagesCreatine Kinase: NAC. Kinetic UV. LiquidJorge PinedaNo ratings yet
- ATCaseDocument24 pagesATCaseRomi GeorgeNo ratings yet
- Pone 0112963 s006Document6 pagesPone 0112963 s006sadiamushtaq822No ratings yet
- Cumene Process DesignDocument16 pagesCumene Process Designendang dian lestariNo ratings yet
- NRL Price List 2018Document17 pagesNRL Price List 2018Anonymous YS9NbuNo ratings yet
- Signature Assignment 4 Central Dogma 1Document5 pagesSignature Assignment 4 Central Dogma 1api-709276885No ratings yet
- Aspergillus Oryzae Laea Regulates Kojic Acid Synthesis Genes PDFDocument4 pagesAspergillus Oryzae Laea Regulates Kojic Acid Synthesis Genes PDFBich Phuong NguyenNo ratings yet
- Supplementary Table 1. A Full List of Cancer GenesDocument685 pagesSupplementary Table 1. A Full List of Cancer GenesFaruque HossainNo ratings yet
- myDNA Comprehensive Health Report Sample Gene List March 2023 New SNPsDocument6 pagesmyDNA Comprehensive Health Report Sample Gene List March 2023 New SNPsCarleta StanNo ratings yet
- Signature Assignment 4 Central DogmaDocument6 pagesSignature Assignment 4 Central Dogmaapi-631586093No ratings yet
- Aug 2021Document9 pagesAug 2021Niharika LallNo ratings yet
- Dhande RatesDocument25 pagesDhande Ratessudhir dNo ratings yet
- Got Ast Beis38 02-2011Document2 pagesGot Ast Beis38 02-2011Guneyden GuneydenNo ratings yet
- Fluid ElektrolitDocument63 pagesFluid ElektrolitsyifaNo ratings yet
- Cyanexpert 130: Application SheetsDocument55 pagesCyanexpert 130: Application Sheets林圣贺No ratings yet
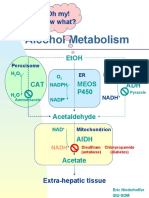
- Alcohol Metabolism: Oh My! Now What?Document5 pagesAlcohol Metabolism: Oh My! Now What?pranjlNo ratings yet
- Signature Assignment 4 Central DogmaDocument6 pagesSignature Assignment 4 Central Dogmaapi-724481252No ratings yet
- Erba SGPTDocument2 pagesErba SGPTAnil Kumar67% (3)
- Bumetanide Torsemide: Desmopressin - V2Document1 pageBumetanide Torsemide: Desmopressin - V2med testNo ratings yet
- Exercise MetabolismDocument1 pageExercise MetabolismLew MingNo ratings yet
- Protein Biosynthesis in Eukaryotes: Prepared By: Pramod K.C Roll No: 15 Bachelor in Pharmacy Second YearDocument29 pagesProtein Biosynthesis in Eukaryotes: Prepared By: Pramod K.C Roll No: 15 Bachelor in Pharmacy Second YearPramod KcNo ratings yet
- Diluent ISE Module Cleaner Solution ISE Module Urine Diluent Cuvette Extra Wash Solution Probe Extra Wash SolutionDocument4 pagesDiluent ISE Module Cleaner Solution ISE Module Urine Diluent Cuvette Extra Wash Solution Probe Extra Wash SolutionAnt WonNo ratings yet
- Konelab PRIME 30iDocument6 pagesKonelab PRIME 30iSayed HasnainNo ratings yet
- SL No Tast Name PriceDocument6 pagesSL No Tast Name Pricesmrutiranjan paridaNo ratings yet
- d1d5c SNP Molecular Genetics New Ver 30102017Document17 pagesd1d5c SNP Molecular Genetics New Ver 30102017Harun GanićNo ratings yet
- Aspect To Consider in Fluid TherapyDocument34 pagesAspect To Consider in Fluid TherapyhanifahNo ratings yet
- Bio, CyclesDocument15 pagesBio, CyclesyoussefbeniameenNo ratings yet
- Run2 Fix Result 05122021 38166-38181Document2 pagesRun2 Fix Result 05122021 38166-38181Hiskia rambeNo ratings yet
- Nutrients SensingDocument5 pagesNutrients SensingPriyanka DasNo ratings yet
- Fluids & ElectrolytesDocument18 pagesFluids & ElectrolytesBiway RegalaNo ratings yet
- RNAi Drug ListDocument26 pagesRNAi Drug ListCarrieNo ratings yet
- 2021 - A Two in On Strategy SupplementaryDocument12 pages2021 - A Two in On Strategy SupplementaryMay Htet AungNo ratings yet
- Full WWPDB X-Ray Structure Validation Report: May 16, 2020 12:57 PM BSTDocument23 pagesFull WWPDB X-Ray Structure Validation Report: May 16, 2020 12:57 PM BSTAlex Enrique Acosta RamosNo ratings yet
- TryptophanDocument4 pagesTryptophanAmit AnirudhNo ratings yet
- 5BBB0223 Metabolic Integration PSW1 ExplanationDocument25 pages5BBB0223 Metabolic Integration PSW1 ExplanationW BNo ratings yet
- PNTD 0009421 s001Document1 pagePNTD 0009421 s001MehranMalekiNo ratings yet
- The RNA Codons: Arlegui, Ronnel A. MTW-11:30AM-12:30PM Bsn-Ii-F Biochemistry LectureDocument4 pagesThe RNA Codons: Arlegui, Ronnel A. MTW-11:30AM-12:30PM Bsn-Ii-F Biochemistry LecturePaul Orly FerrerNo ratings yet
- Ejercicios de La Beta OxidaciónDocument2 pagesEjercicios de La Beta Oxidaciónwalkyria camargoNo ratings yet
- Instruction Set of 8051Document3 pagesInstruction Set of 8051revanthNo ratings yet
- Bio PlasticDocument15 pagesBio PlasticAkhil RautelaNo ratings yet
- Lyphochek Assayed Chemistry Control: Bio-Rad LaboratoriesDocument2 pagesLyphochek Assayed Chemistry Control: Bio-Rad LaboratoriesTarunNo ratings yet
- Metabolisme As - AminoDocument24 pagesMetabolisme As - AminoRegatta Ringga Hanessa PutryNo ratings yet
- Protein Sequenching: Protein and Dna-Based Information Technology (WEEK 9)Document14 pagesProtein Sequenching: Protein and Dna-Based Information Technology (WEEK 9)CSERM UNASNo ratings yet
- Blood Urine Test Total ErodeDocument50 pagesBlood Urine Test Total Erodealaudeen2014No ratings yet
- 01-Revisi 03-2022 Tarif SumateraDocument26 pages01-Revisi 03-2022 Tarif SumateraAmelia Prity SyaniNo ratings yet
- En ZymologyDocument6 pagesEn ZymologyNathaniel Derige AndesNo ratings yet
- Beste Summary Ever BiochemDocument125 pagesBeste Summary Ever BiochemViktoriyaNo ratings yet
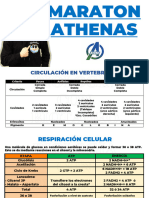
- Maraton AthenasDocument27 pagesMaraton Athenassmitjerry206No ratings yet
- Pricelist NewmeganeDocument5 pagesPricelist NewmeganeMilun MarkovicNo ratings yet
- CRM Price List 2017: Mark Codes ExplanationDocument12 pagesCRM Price List 2017: Mark Codes ExplanationRhegy PranandaNo ratings yet
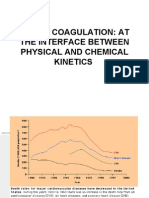
- Blood Coagulation: at The Interface Between Physical and Chemical KineticsDocument43 pagesBlood Coagulation: at The Interface Between Physical and Chemical Kineticsdaw022No ratings yet
- GPT Alt Beis36 02-2011Document2 pagesGPT Alt Beis36 02-2011sazzadsazibNo ratings yet
- Lecture 22 11-17-22Document19 pagesLecture 22 11-17-22Caleb HeNo ratings yet
- BC CH - 22Document56 pagesBC CH - 22FlorangNo ratings yet
- PathophysiologyDocument1 pagePathophysiologyFafa MusNo ratings yet
- Handbook of Palladium-Catalysed Organic ReactionsFrom EverandHandbook of Palladium-Catalysed Organic ReactionsJ. C. FiaudNo ratings yet
- Neonatalcholestasis by by Dr. Dedi, SpADocument41 pagesNeonatalcholestasis by by Dr. Dedi, SpAarvaniaNo ratings yet
- Daftar Pustaka 03Document3 pagesDaftar Pustaka 03arvaniaNo ratings yet
- Feeding Disorders - Blok 16Document65 pagesFeeding Disorders - Blok 16arvaniaNo ratings yet
- Cyanotic Spell: Dr. Shirley L A, Sp. A 12 April 2011Document6 pagesCyanotic Spell: Dr. Shirley L A, Sp. A 12 April 2011Kahfi Rakhmadian KiraNo ratings yet
- Evaluation of The Child With Global Developmental Delay (GDD)Document5 pagesEvaluation of The Child With Global Developmental Delay (GDD)Magdalena Dwiyani HutajuluNo ratings yet
- Caribbean Coral Reefs - Status Report 1970-2012 PDFDocument306 pagesCaribbean Coral Reefs - Status Report 1970-2012 PDFbutterflybreNo ratings yet
- Medical History FormatDocument5 pagesMedical History Formatkrzia TehNo ratings yet
- Overview On Cucurbita MaximaDocument4 pagesOverview On Cucurbita MaximaIRFAN KurniawanNo ratings yet
- Ainu Illness&healingDocument21 pagesAinu Illness&healingRaluca MoiseNo ratings yet
- Tracheoesophageal Fistula: DR - Yamuna TulasiDocument59 pagesTracheoesophageal Fistula: DR - Yamuna TulasiTulasiNo ratings yet
- Pentra 60Document308 pagesPentra 60Leonardo M. MonteiroNo ratings yet
- Pest and Disease of RiceDocument19 pagesPest and Disease of RiceRosevi Venida TotanesNo ratings yet
- OPTH 118409 Undesirable Systemic Side Effects of Ophthalmic Drops From T 120716Document9 pagesOPTH 118409 Undesirable Systemic Side Effects of Ophthalmic Drops From T 120716Optm Abdul AzizNo ratings yet
- Circular ExcisionDocument2 pagesCircular ExcisionIde Bagoes InsaniNo ratings yet
- Tooth Movement (Frontiers of Oral Biology)Document92 pagesTooth Movement (Frontiers of Oral Biology)GABRIELA NIETO GONZALEZNo ratings yet
- PNPA Application Form 2010Document2 pagesPNPA Application Form 2010Jenny Rose Imperial Castillo-Aragon100% (2)
- 483 FullDocument9 pages483 FullLucianaNo ratings yet
- NCM 101 Health AssessmentDocument7 pagesNCM 101 Health AssessmentCristoper Bodiongan100% (1)
- Multiple MyelomaDocument28 pagesMultiple MyelomaBHAGYASHREE SHELAR100% (2)
- Procedures - Sharps Management and Injury ProtocolDocument6 pagesProcedures - Sharps Management and Injury ProtocolMarwan GamaleldinNo ratings yet
- Carcinosin SCDocument10 pagesCarcinosin SCnitkolNo ratings yet
- DT - Normal Eyes With Sudden Painless Loss of VisionDocument34 pagesDT - Normal Eyes With Sudden Painless Loss of VisionIzzatul Yazidah100% (1)
- 中英對照讀新聞Document55 pages中英對照讀新聞AZsun100% (2)
- The Truth About DyslexiaDocument2 pagesThe Truth About DyslexiaLinda BalsigerNo ratings yet
- What Do You Do in Your Free Time?: Lesson C Being HealthyDocument2 pagesWhat Do You Do in Your Free Time?: Lesson C Being HealthyJaimeNo ratings yet
- NP1 Drill W RationaleDocument19 pagesNP1 Drill W RationaleCarlos, Angeline J.No ratings yet
- Case Study (Typhoid Fever)Document2 pagesCase Study (Typhoid Fever)lance rowyNo ratings yet
- Apostila de InglêsDocument28 pagesApostila de InglêsBruno AlvesNo ratings yet
- Abby Randi NepalDocument11 pagesAbby Randi NepalAbbyNo ratings yet
- Patient NCPDocument8 pagesPatient NCPlouie john abilaNo ratings yet
- Brain Heart "Cross-Talk" in Traumatic Brain InjuryDocument121 pagesBrain Heart "Cross-Talk" in Traumatic Brain InjuryHamilton Jr da LisaneNo ratings yet