You might also like
- Clinical Pharmacokinetics 2013Document68 pagesClinical Pharmacokinetics 2013Law YouNo ratings yet
- Pharmacology Illustrated Notes: Calcium Channel Blockers and DigoxinDocument148 pagesPharmacology Illustrated Notes: Calcium Channel Blockers and DigoxinShikha Khemani88% (8)
- Pharm NotesDocument198 pagesPharm NotesNancy Danielz80% (5)
- Drugs Cards 208Document11 pagesDrugs Cards 208SOOOS94100% (3)
- PharmacokineticsDocument112 pagesPharmacokineticsGog Rg100% (2)
- Lexicomp Handbooks CatalogDocument12 pagesLexicomp Handbooks CatalogferiskaNo ratings yet
- Cholinergic Agonists and AntagonistsDocument21 pagesCholinergic Agonists and Antagonistsjheannie02100% (3)
- Pharmacology of Autonomic Nervous SystemDocument106 pagesPharmacology of Autonomic Nervous Systemoscar3spurgeonNo ratings yet
- Pain Physiology Pathways Mechanisms ClassificationDocument71 pagesPain Physiology Pathways Mechanisms Classificationkeerthi_keshapagaNo ratings yet
- The role of histamine in pharmacology and its antagonistsDocument21 pagesThe role of histamine in pharmacology and its antagonistsMartina Alarcon Acevedo100% (1)
- Drug Interactions HandoutDocument5 pagesDrug Interactions HandoutBhavin DesaiNo ratings yet
- ANS Pharmacology-Cholinergic AgentsDocument55 pagesANS Pharmacology-Cholinergic AgentsMarc Imhotep Cray, M.D.No ratings yet
- Flower EsscencesDocument2 pagesFlower EsscencesDivyajyoti DevaNo ratings yet
- Pharmacology Mock Exam MCQDocument8 pagesPharmacology Mock Exam MCQanaeshklNo ratings yet
- Pharma 1.2 - Pharmacokinetics (Vision) PDFDocument14 pagesPharma 1.2 - Pharmacokinetics (Vision) PDFVon Javier GamateroNo ratings yet
- SympathomimeticsDocument25 pagesSympathomimeticsMirza Shaharyar BaigNo ratings yet
- Cholinergic Agonists: Dr. Mohamed Samai BSC (Hons), MSC, MBBS, PGCRM, PHD Head, Department of Pharmacology Comahs, UslDocument31 pagesCholinergic Agonists: Dr. Mohamed Samai BSC (Hons), MSC, MBBS, PGCRM, PHD Head, Department of Pharmacology Comahs, Uslmatchees-gone rogue100% (1)
- Adrenergics & Adrenergic BlockersDocument5 pagesAdrenergics & Adrenergic Blockersapi-3739910100% (4)
- Initial Assessment and Management of Trauma PatientsDocument8 pagesInitial Assessment and Management of Trauma PatientsAlvin De LunaNo ratings yet
- Pharmacology notes on adrenergic agonists and antagonistsDocument3 pagesPharmacology notes on adrenergic agonists and antagonistsMohd Afiq AizuddinNo ratings yet
- Endocrine PharmacologyDocument42 pagesEndocrine PharmacologyAhmed El SharkawyNo ratings yet
- Topic 2 - Adrenergic DrugsDocument52 pagesTopic 2 - Adrenergic DrugsAngeli Gregorio100% (1)
- Skeletal Muscle RelaxantsDocument30 pagesSkeletal Muscle Relaxantsmatchees-gone rogueNo ratings yet
- Pharmacology - Git DrugsDocument123 pagesPharmacology - Git DrugsBenjamin Joel Breboneria75% (4)
- Cholinergic Antagonists "Anticholinergic Drugs" (ParasympatholyticsDocument32 pagesCholinergic Antagonists "Anticholinergic Drugs" (ParasympatholyticsmiznahNo ratings yet
- Cell Wall InhibitorsDocument52 pagesCell Wall InhibitorsApurba Sarker Apu100% (1)
- Cholinergic Anticholinergic DrugsDocument60 pagesCholinergic Anticholinergic DrugsMD. RASEL MAHMUD MIMNo ratings yet
- CSCU Module 11 Security On Social Networking Sites PDFDocument34 pagesCSCU Module 11 Security On Social Networking Sites PDFSandeep Roy100% (2)
- CSCU Module 13 Securing Mobile Devices PDFDocument50 pagesCSCU Module 13 Securing Mobile Devices PDFSandeep Roy100% (2)
- Lecture - 1 Introduction To PharmacologyDocument62 pagesLecture - 1 Introduction To PharmacologyAshique FarhadNo ratings yet
- ANS-Pharmacology Adrenergic DrugsDocument65 pagesANS-Pharmacology Adrenergic DrugsMarc Imhotep Cray, M.D.75% (4)
- Types of Medications Used After SurgeryDocument9 pagesTypes of Medications Used After SurgeryRegine VillanuevaNo ratings yet
- An Introduction to Pharmacology: A Tutorial Study GuideFrom EverandAn Introduction to Pharmacology: A Tutorial Study GuideRating: 3 out of 5 stars3/5 (2)
- Parasympathetic Pharmacology Drugs Muscarine and Nicotinic RecpetorsDocument56 pagesParasympathetic Pharmacology Drugs Muscarine and Nicotinic RecpetorsMatthewNo ratings yet
- Introduction To Pharmacology - Prescribing - FastbleepDocument12 pagesIntroduction To Pharmacology - Prescribing - FastbleepSareeya ShreNo ratings yet
- Therapeutic Drug Monitoring: By: Adewale Akinseloyin Oluwatimilehin Agboola Oluwatosin AjibadeDocument33 pagesTherapeutic Drug Monitoring: By: Adewale Akinseloyin Oluwatimilehin Agboola Oluwatosin AjibadeJoe AjibadeNo ratings yet
- Data Structure Lab ManualDocument39 pagesData Structure Lab ManualbharatkumarpadhiNo ratings yet
- Introduction to Autonomic PharmacologyDocument24 pagesIntroduction to Autonomic PharmacologyChacha ChachaNo ratings yet
- Pre AnaestheticsDocument69 pagesPre AnaestheticsPraney SlathiaNo ratings yet
- Osseointegration Short Review PDFDocument5 pagesOsseointegration Short Review PDFkryptonites1234No ratings yet
- CSCU Module 09 Securing Email Communications PDFDocument42 pagesCSCU Module 09 Securing Email Communications PDFSandeep Roy100% (3)
- CSCU Module 09 Securing Email Communications PDFDocument42 pagesCSCU Module 09 Securing Email Communications PDFSandeep Roy100% (3)
- Pharmacology of Adrenergic AgonistsDocument9 pagesPharmacology of Adrenergic Agonistsfiena92No ratings yet
- CSCU Module 10 Social Engineering and Identity Theft PDFDocument42 pagesCSCU Module 10 Social Engineering and Identity Theft PDFSandeep Roy100% (1)
- CSCU Module 10 Social Engineering and Identity Theft PDFDocument42 pagesCSCU Module 10 Social Engineering and Identity Theft PDFSandeep Roy100% (1)
- CSCU Module 12 Information Security and Legal Compliance PDFDocument12 pagesCSCU Module 12 Information Security and Legal Compliance PDFSandeep Roy100% (1)
- CSCU Module 05 Data Backup and Disaster Recovery PDFDocument51 pagesCSCU Module 05 Data Backup and Disaster Recovery PDFSandeep Roy100% (5)
- CSCU Module 06 Internet Security PDFDocument79 pagesCSCU Module 06 Internet Security PDFSandeep Roy67% (3)
- CSCU Module 06 Internet Security PDFDocument79 pagesCSCU Module 06 Internet Security PDFSandeep Roy67% (3)
- CSCU Module 04 Data Encryption PDFDocument23 pagesCSCU Module 04 Data Encryption PDFSandeep Roy100% (1)
- CSCU Module 04 Data Encryption PDFDocument23 pagesCSCU Module 04 Data Encryption PDFSandeep Roy100% (1)
- CSCU Module 07 Securing Network Connections PDFDocument60 pagesCSCU Module 07 Securing Network Connections PDFSandeep Roy100% (2)
- CSCU Module 02 Securing Operating Systems PDFDocument77 pagesCSCU Module 02 Securing Operating Systems PDFSandeep Roy100% (3)
- CSCU Module 03 Protecting Systems Using Antiviruses PDFDocument32 pagesCSCU Module 03 Protecting Systems Using Antiviruses PDFSandeep Roy100% (3)
- CSCU Module 01 Foundations of SecurityDocument25 pagesCSCU Module 01 Foundations of SecurityAli Imron75% (4)
- CSCU Module 01 Foundations of SecurityDocument25 pagesCSCU Module 01 Foundations of SecurityAli Imron75% (4)
- Cholinergic DrugsDocument32 pagesCholinergic DrugsApt FianNo ratings yet
- Adrenergic AgentsDocument57 pagesAdrenergic AgentsAn Lo100% (1)
- Cholinergic AgonistsDocument25 pagesCholinergic AgonistsRahul VadlapatlaNo ratings yet
- Pharmacology and PrescriptionDocument184 pagesPharmacology and PrescriptiontiffylolaNo ratings yet
- Pharmacodynamics BDS97Document42 pagesPharmacodynamics BDS97Dr.U.P.Rathnakar.MD.DIH.PGDHM100% (2)
- Antiplatelet and Thrombolytic DrugsDocument48 pagesAntiplatelet and Thrombolytic DrugsNofa PuspitaNo ratings yet
- Introduction To Cns PharmacologyDocument66 pagesIntroduction To Cns PharmacologyYazan Emad Salem100% (1)
- Cholinergic and AnticholinergicDocument77 pagesCholinergic and Anticholinergicsweta sumanNo ratings yet
- Pharmacokinetics lecture notes on absorption, distribution, metabolism, and excretion (ADMEDocument4 pagesPharmacokinetics lecture notes on absorption, distribution, metabolism, and excretion (ADMEfaithsheepNo ratings yet
- Pharmacology: Core Curriculum in NephrologyDocument11 pagesPharmacology: Core Curriculum in NephrologyYuppie RajNo ratings yet
- General Pharmacology-QuestionDocument4 pagesGeneral Pharmacology-Questionlina amjadNo ratings yet
- Drug Interactions of Antianginal Drugs..Document40 pagesDrug Interactions of Antianginal Drugs..Kamal SikandarNo ratings yet
- Neuromuscular BlockersDocument25 pagesNeuromuscular BlockersAbdelrahman GalalNo ratings yet
- 3 NeurotransmissionDocument31 pages3 Neurotransmissionsarahcho12152No ratings yet
- Autonomic Nervous System: Parasympathetic and Sympathetic DivisionsDocument107 pagesAutonomic Nervous System: Parasympathetic and Sympathetic DivisionsMaria Mercedes LeivaNo ratings yet
- (OS 213) LEC 03 Drugs Acting On The Respiratory System (1) - 1Document16 pages(OS 213) LEC 03 Drugs Acting On The Respiratory System (1) - 1Yavuz DanisNo ratings yet
- Cholinergics and Cholinergic BlockersDocument5 pagesCholinergics and Cholinergic Blockersapi-3739910100% (3)
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- 6.3 Defence Against Infectious DiseaseDocument43 pages6.3 Defence Against Infectious DiseaseAlacrity Xenoion SpadesNo ratings yet
- (DownSub - Com) Pharmacology - PHARMACOKINETICS (MADE EASY)Document8 pages(DownSub - Com) Pharmacology - PHARMACOKINETICS (MADE EASY)Stephen VuelbanNo ratings yet
- General Pharmacology - Sources of Drugs and Routes of AdministrationDocument48 pagesGeneral Pharmacology - Sources of Drugs and Routes of AdministrationDhriti Brahma78% (9)
- (CL15) Cholinergic and Anticholinergic Agentscholinergic and Anticholinergic Agents - ImaDocument41 pages(CL15) Cholinergic and Anticholinergic Agentscholinergic and Anticholinergic Agents - ImaRahman Anwar100% (1)
- Anaesthetic Drug TablesDocument6 pagesAnaesthetic Drug TablesNanaNo ratings yet
- General AnestheticsDocument36 pagesGeneral AnestheticsnidyaNo ratings yet
- Antibiotics: Means Against LifeDocument13 pagesAntibiotics: Means Against Lifeshankul kumar100% (1)
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Types of GDDocument1 pageTypes of GDsachinthestar20079057No ratings yet
- Data Structure Lab - MCA16-LDocument57 pagesData Structure Lab - MCA16-Lapi-3732063No ratings yet
- Data Structures With C LabDocument40 pagesData Structures With C LabPradeep Gowda100% (2)
- Data Structures PDFDocument515 pagesData Structures PDFzahiid munirNo ratings yet
- Data Structure Lab ProgramsDocument26 pagesData Structure Lab Programsnofeelingrahul100% (3)
- ProposalsDocument7 pagesProposalsSandeep RoyNo ratings yet
- ListeningDocument7 pagesListeningSandeep RoyNo ratings yet
- Swot Analysis in CommunicationDocument5 pagesSwot Analysis in CommunicationSandeep RoyNo ratings yet
- Presentation SkillsDocument11 pagesPresentation SkillsSandeep RoyNo ratings yet
- Group Discussion Techniques and Strategies (35 charactersDocument9 pagesGroup Discussion Techniques and Strategies (35 charactersSandeep RoyNo ratings yet
- BCA New SyllabusDocument19 pagesBCA New Syllabussiddhartha ray100% (2)
- Weekly Epi Update 79Document19 pagesWeekly Epi Update 79Lee Ji EunNo ratings yet
- HIV RNA Virus Classification and PathogenesisDocument2 pagesHIV RNA Virus Classification and PathogenesisBONNA FAYE CHRISZEL HUI YING TANNo ratings yet
- Nonadherence To Medications Among Persons With Bipolar Affective Disorder - A ReviewDocument9 pagesNonadherence To Medications Among Persons With Bipolar Affective Disorder - A ReviewIra DomunNo ratings yet
- Preguntas de Investigación Priorizadas en Salud Mental PDFDocument10 pagesPreguntas de Investigación Priorizadas en Salud Mental PDFMatiasZambranoCNo ratings yet
- Cervical Cancer: The Silent KillerDocument19 pagesCervical Cancer: The Silent KillerDennis CosmodNo ratings yet
- COVID-19 Pneumonia in Children: From Etiology To ManagementDocument8 pagesCOVID-19 Pneumonia in Children: From Etiology To Managementnugraha sultanNo ratings yet
- TechTalk Sodium CitrateDocument2 pagesTechTalk Sodium Citrated40sithui50% (2)
- Nervous SystemDocument49 pagesNervous SystemVinDiesel Balag-eyNo ratings yet
- Brochura UrgoTul AGDocument4 pagesBrochura UrgoTul AGDaniguedesNo ratings yet
- Effect of Steam Inhalation On Nasal Mucociliary Clearance in Normal Individuals and Nasal Disease Sta PDFDocument3 pagesEffect of Steam Inhalation On Nasal Mucociliary Clearance in Normal Individuals and Nasal Disease Sta PDFyolandaNo ratings yet
- Merge-Davao (Multi - Educational Review Group Experts) : Physiological IntegrityDocument12 pagesMerge-Davao (Multi - Educational Review Group Experts) : Physiological IntegrityNom NomNo ratings yet
- Kiara WhitakerDocument2 pagesKiara Whitakerapi-267218383No ratings yet
- Arthrex ACP® Double SyringeDocument8 pagesArthrex ACP® Double SyringeMofit penjačka stijenaNo ratings yet
- Folliculitis Decalvans Update July 2019 - Lay Reviewed July 2019Document4 pagesFolliculitis Decalvans Update July 2019 - Lay Reviewed July 2019sjeyarajah21No ratings yet
- Autopsy Who Peforms The Autopsy?: Aut-+ Opsis Sight, Appearance - More at OpticDocument5 pagesAutopsy Who Peforms The Autopsy?: Aut-+ Opsis Sight, Appearance - More at Opticmiguel gaquitNo ratings yet
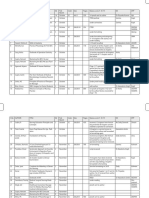
- St. Anthony College Calapan City, Inc. Bayanan I, Calapan CityDocument3 pagesSt. Anthony College Calapan City, Inc. Bayanan I, Calapan CityMike Faustino SolangonNo ratings yet
- ICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular HypertrophyDocument5 pagesICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular Hypertrophysamir raflaNo ratings yet
- Inhalation InjuriesDocument4 pagesInhalation InjuriesMohammadAwitNo ratings yet
- Health and Safety Solutions Accident Investigation FormDocument2 pagesHealth and Safety Solutions Accident Investigation Formhussein aliNo ratings yet
- W3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Document22 pagesW3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Rona DindangNo ratings yet
- NeuropsychiatricDocument18 pagesNeuropsychiatricSamuel JohnsonNo ratings yet
- Drug Abuse Essay - AlcoholismDocument5 pagesDrug Abuse Essay - Alcoholismapi-509288017No ratings yet
- Firs World Report PDFDocument35 pagesFirs World Report PDFMarv MarvNo ratings yet
- Untitled 5 PDFDocument6 pagesUntitled 5 PDFDeepak saxenaNo ratings yet