You might also like
- EKG/ECG Study GuideDocument13 pagesEKG/ECG Study GuideSherree HayesNo ratings yet
- 6.2 Nervous CoordinationDocument1 page6.2 Nervous CoordinationRS JNo ratings yet
- Optical Sampling Transient Analyzer (OSTA) System (IEEE Journal of Quantum Electronics, Vol. 11, Issue 9) (1975)Document1 pageOptical Sampling Transient Analyzer (OSTA) System (IEEE Journal of Quantum Electronics, Vol. 11, Issue 9) (1975)nirajchat1991No ratings yet
- Arterial Pulse Recording & Interpretation GuideDocument5 pagesArterial Pulse Recording & Interpretation GuideHarisree SNo ratings yet
- Arrhythmia 2021-2022 Semester 1Document42 pagesArrhythmia 2021-2022 Semester 1Omar AlaamNo ratings yet
- Orthdromic Vs Antidromic SVT, and Why It MattersDocument1 pageOrthdromic Vs Antidromic SVT, and Why It MattersHenry Leroy Lewis BatresNo ratings yet
- Electrocardiograpy - 0Document9 pagesElectrocardiograpy - 0Sakshi ChoudharyNo ratings yet
- Sistema de ConduccionDocument5 pagesSistema de Conduccionapi-543828470No ratings yet
- Neuron Action Potentials - The Creation of A Brain Signal (Article) - Khan AcademyDocument21 pagesNeuron Action Potentials - The Creation of A Brain Signal (Article) - Khan Academymohammed awolNo ratings yet
- Conexinas y Nodo AV. Heart Rhythm 2013Document8 pagesConexinas y Nodo AV. Heart Rhythm 2013Ernesto J. Rocha ReyesNo ratings yet
- VII-PHYSIOLOGY - Kaplan Medical USMLE Step 1 Lecture Notes 2021 (2021) (Arrastrado)Document1 pageVII-PHYSIOLOGY - Kaplan Medical USMLE Step 1 Lecture Notes 2021 (2021) (Arrastrado)Beto RendonNo ratings yet
- Cardiac Rhythm Disorders: The Human HeartDocument26 pagesCardiac Rhythm Disorders: The Human HeartLena LengNo ratings yet
- Chapter 9Document28 pagesChapter 9Jill ZabalaNo ratings yet
- CVS - K3 - FS - Cardiovascular System Without SoundDocument20 pagesCVS - K3 - FS - Cardiovascular System Without SoundE. Tito Julianda SinagaNo ratings yet
- Doidera EEGDocument17 pagesDoidera EEGLuís PachecoNo ratings yet
- Saltatory Conduction: Action Potential "HoppingDocument9 pagesSaltatory Conduction: Action Potential "HoppingNantha KumarNo ratings yet
- Brain Arteriovenous Malforamtion: Dr. Suresh Bishokarma MS, MCH (Neurosurgery)Document95 pagesBrain Arteriovenous Malforamtion: Dr. Suresh Bishokarma MS, MCH (Neurosurgery)rr_eeyNo ratings yet
- ECG Heart SignalDocument109 pagesECG Heart SignalSk. Laila AyeshaNo ratings yet
- ECG and Einthoven's Triangle Flashcards - QuizletDocument5 pagesECG and Einthoven's Triangle Flashcards - QuizletMr. DybalaNo ratings yet
- Online ultrasound study guideDocument7 pagesOnline ultrasound study guideSarath kumarNo ratings yet
- Instantaneous neural signal transmissionDocument78 pagesInstantaneous neural signal transmissionana luNo ratings yet
- ElectrocardiogramDocument2 pagesElectrocardiogramonijinoNo ratings yet
- 6 - NM2 Action PotentialDocument48 pages6 - NM2 Action Potentialraphaelyohana140No ratings yet
- CardiacArrhythmiasPathophysiology PDFDocument1 pageCardiacArrhythmiasPathophysiology PDFNeelam Raj ThakurNo ratings yet
- Marinedrugs 15 00295Document16 pagesMarinedrugs 15 00295Jean Pierre Chastre LuzaNo ratings yet
- Sistema de Conduccion Karen Daniela VelascoDocument3 pagesSistema de Conduccion Karen Daniela Velascoapi-540316757No ratings yet
- Excitation of HeartDocument9 pagesExcitation of Heartemir krlpNo ratings yet
- MED II 1.01-ECG-and-Arrythmia-RecognitionDocument40 pagesMED II 1.01-ECG-and-Arrythmia-RecognitionCRUZ Jill EraNo ratings yet
- ECG basics: How to read an electrocardiogramDocument6 pagesECG basics: How to read an electrocardiogramBanana PeachNo ratings yet
- Critical Care: ElectrophysiologyDocument180 pagesCritical Care: ElectrophysiologyArianne Joy C. TamarayNo ratings yet
- Sense OrgansDocument3 pagesSense OrgansAabhaNo ratings yet
- Mechanical and Electrical Events of The Caridac Cycle: Hetal Gohil Mmed Paediatric Surgery Facilitated by DR BukachiDocument24 pagesMechanical and Electrical Events of The Caridac Cycle: Hetal Gohil Mmed Paediatric Surgery Facilitated by DR BukachiJustine NyangaresiNo ratings yet
- chap16Document35 pageschap16jim.68.richtNo ratings yet
- Biophypsy M1L3Document3 pagesBiophypsy M1L3Maria Helen PalacayNo ratings yet
- Rolling On GroundDocument7 pagesRolling On GroundJawad HameedNo ratings yet
- DNA and Cell Resonance: How Magnetic Waves Enable Cell CommunicationDocument6 pagesDNA and Cell Resonance: How Magnetic Waves Enable Cell CommunicationmedellincolombiaNo ratings yet
- SemiconductorDocument3 pagesSemiconductorNitin RanaNo ratings yet
- A234 ElectrocardiogramsDocument4 pagesA234 Electrocardiogramsramloghun veerNo ratings yet
- CCN Lab (Feu)Document37 pagesCCN Lab (Feu)Ashley Nicole LimNo ratings yet
- 12 Strand DNA Morphogenetic Engineering Via Holofractal Morphogenetic Reprogramming of Genetic InformationDocument14 pages12 Strand DNA Morphogenetic Engineering Via Holofractal Morphogenetic Reprogramming of Genetic InformationJNo ratings yet
- Aritmia PDFDocument114 pagesAritmia PDFRhahima SyafrilNo ratings yet
- Paced RhytmsDocument16 pagesPaced RhytmsTor JaNo ratings yet
- EKG Study Guide: Anatomy of The HeartDocument28 pagesEKG Study Guide: Anatomy of The HeartGrasiela CampbellNo ratings yet
- Junctional: TachycardiaDocument11 pagesJunctional: TachycardiachaiNo ratings yet
- Nerve Physiology: - 4. GeneticDocument9 pagesNerve Physiology: - 4. Geneticashley nicholeNo ratings yet
- NROSCI 1012 - Lecture 22Document4 pagesNROSCI 1012 - Lecture 22HonzaNo ratings yet
- Paper. Action-Potentials-Generation-and-propagation 1Document8 pagesPaper. Action-Potentials-Generation-and-propagation 1Mike NundweNo ratings yet
- Parallel Fibre Purkinje Cell B Cerebellum: What Adjusts The VOR?Document1 pageParallel Fibre Purkinje Cell B Cerebellum: What Adjusts The VOR?GASA1111No ratings yet
- 48 Lecture ShortDocument48 pages48 Lecture ShortNoahNo ratings yet
- DYSRHYTMIASDocument13 pagesDYSRHYTMIASApple Mae AlmoniaNo ratings yet
- RC - Artifacts TableDocument11 pagesRC - Artifacts TableAaron SmithNo ratings yet
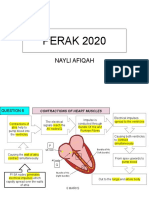
- Essay Bio Nayli PERAK 2020Document6 pagesEssay Bio Nayli PERAK 2020HAMIRAH ABD HAMIDNo ratings yet
- Ecg Skills LabDocument7 pagesEcg Skills Labmelba040510No ratings yet
- 30 34Document37 pages30 34Siva KumarNo ratings yet
- Interference of Acoustic Waves, Stationary Waves and Diffraction at A Slot With PC IntDocument7 pagesInterference of Acoustic Waves, Stationary Waves and Diffraction at A Slot With PC IntJose GalvanNo ratings yet
- ECG Anatomy and Physiology GuideDocument16 pagesECG Anatomy and Physiology Guide12Klaire Therese CabigasNo ratings yet
- 2.Nerve PhysiologyDocument43 pages2.Nerve Physiologycongresarad2022No ratings yet
- Nervous System Part 1Document11 pagesNervous System Part 1Mariel AbatayoNo ratings yet
- Plasma Astrophysics: International Series of Monographs in Natural PhilosophyFrom EverandPlasma Astrophysics: International Series of Monographs in Natural PhilosophyNo ratings yet
- TBI Research DirectoryDocument330 pagesTBI Research Directorybradfordmccall1No ratings yet
- pedCAT BrochureDocument12 pagespedCAT BrochureVinti Singh100% (1)
- Drug Affecting Cardiovascular FunctionDocument21 pagesDrug Affecting Cardiovascular Functionnurliah armandNo ratings yet
- Ap2 Safe ManipulationDocument5 pagesAp2 Safe ManipulationDarthVader975No ratings yet
- A Brief Reiki HistoryDocument3 pagesA Brief Reiki HistoryShubham InfinityNo ratings yet
- Marketing Management Caselets 15102009Document13 pagesMarketing Management Caselets 15102009sreeramkannan285475% (4)
- Functional Food DevelopmentDocument11 pagesFunctional Food Developmentlaura restrepoNo ratings yet
- Four Types of Pulse Oximeters Accurately Detect Hypoxia During Low Perfusion and MotionDocument11 pagesFour Types of Pulse Oximeters Accurately Detect Hypoxia During Low Perfusion and MotionAldryn MuskananfolaNo ratings yet
- Pencin La Injection 100ml Bar, Coa V f139c Star SpecsDocument3 pagesPencin La Injection 100ml Bar, Coa V f139c Star SpecssajidNo ratings yet
- List of Teaching StaffDocument10 pagesList of Teaching StaffGaurav SinghNo ratings yet
- Root Operations in The Medical and Surgical Section (ICD-10)Document2 pagesRoot Operations in The Medical and Surgical Section (ICD-10)Nicholas HenryNo ratings yet
- Relert Tablets: 1. Qualitative and Quantitative CompositionDocument9 pagesRelert Tablets: 1. Qualitative and Quantitative Compositionddandan_2No ratings yet
- LUMENIS Laser Article on Keloid and Scar Treatment GuidelinesDocument8 pagesLUMENIS Laser Article on Keloid and Scar Treatment GuidelinesAuroraNo ratings yet
- Carpal Tunnel Syndrome - Wikipedia PDFDocument107 pagesCarpal Tunnel Syndrome - Wikipedia PDFMuhammadNo ratings yet
- Quiz MRIDocument7 pagesQuiz MRIMark M. AlipioNo ratings yet
- HEALTH ASSESSMENT!!!Digestive SystemDocument24 pagesHEALTH ASSESSMENT!!!Digestive Systemapi-19885395100% (1)
- CryoglobulinsDocument39 pagesCryoglobulinsanamariavNo ratings yet
- Hospital Case Study FlexsimDocument2 pagesHospital Case Study FlexsimMano KanthanathanNo ratings yet
- Complete Postparturient Uterine Prolapse in HF Cross Bred CowDocument2 pagesComplete Postparturient Uterine Prolapse in HF Cross Bred CowfrankyNo ratings yet
- Good Compounding PracticeDocument5 pagesGood Compounding PracticeRasselle BalangiNo ratings yet
- Care of The Older Adult P1 PointersDocument19 pagesCare of The Older Adult P1 Pointersrica sebabillonesNo ratings yet
- Biomechanics of The Osteoperotic SpineDocument8 pagesBiomechanics of The Osteoperotic SpineIsmael Vara CarvalhoNo ratings yet
- Hema I Chapter 4 - AnticoagDocument16 pagesHema I Chapter 4 - AnticoagderibewNo ratings yet
- Qi Project PaperDocument8 pagesQi Project Paperapi-380333919No ratings yet
- 1989 The Revised Diagnostic Interview Zanarini1989Document9 pages1989 The Revised Diagnostic Interview Zanarini1989Cesar Cantarutti0% (1)
- The Complete Guide To Fixing Your Caveman Posture! The Postural Analysis: Side PostureDocument6 pagesThe Complete Guide To Fixing Your Caveman Posture! The Postural Analysis: Side PostureYouRuggedManlyTypeNo ratings yet
- Kinetics Problem Solving Set7-11.10.15Document13 pagesKinetics Problem Solving Set7-11.10.15Katrina Chan67% (3)
- CSSD Forums Sop 20120716 enDocument73 pagesCSSD Forums Sop 20120716 enNeil Osborne100% (1)
- Clobetasol Propionate Cream, Gel and Ointment Drug InfoDocument7 pagesClobetasol Propionate Cream, Gel and Ointment Drug InfoWhiel Kurt Arzaga SaragconNo ratings yet