You might also like
- Colilithiasis 2Document53 pagesColilithiasis 2Worku KifleNo ratings yet
- Hemorrhoids and Anal ProblemsDocument64 pagesHemorrhoids and Anal ProblemsAhmed Noureldin Ahmed100% (4)
- Abdominal Distention and AscitesDocument49 pagesAbdominal Distention and AscitesNinaNo ratings yet
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisRating: 3 out of 5 stars3/5 (1)
- Biliary Tract Disease - Emmet AndrewsDocument52 pagesBiliary Tract Disease - Emmet AndrewsBoneyJalgarNo ratings yet
- Process Plant Layout - Seán Moran 1-2Document2 pagesProcess Plant Layout - Seán Moran 1-2CunCunAlAndra100% (1)
- Rectal Bleeding OverviewDocument7 pagesRectal Bleeding OverviewYanceHanzieNo ratings yet
- Hemorhhoids CssDocument31 pagesHemorhhoids CssNaren RenNo ratings yet
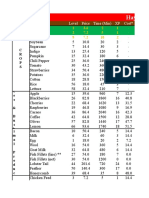
- Hay Day Price Profit AnalysisDocument112 pagesHay Day Price Profit AnalysisCunCunAlAndraNo ratings yet
- Hay Day Price Profit AnalysisDocument112 pagesHay Day Price Profit AnalysisCunCunAlAndraNo ratings yet
- Boards TipsDocument2 pagesBoards TipsElaine June FielNo ratings yet
- Bleeding Per RectumeDocument35 pagesBleeding Per RectumetharakaNo ratings yet
- College of Medicine & Health SciencesDocument56 pagesCollege of Medicine & Health SciencesMebratu DemessNo ratings yet
- Answers To Questions For 2008 CPC Practice ExaminationDocument12 pagesAnswers To Questions For 2008 CPC Practice ExaminationBeverly GraciousNo ratings yet
- Biliary Tract DiseaseDocument52 pagesBiliary Tract DiseaseAna Cotoman100% (1)
- POLYCYTHEMIADocument48 pagesPOLYCYTHEMIAPoova RagavanNo ratings yet
- Ambulance Response Protocol DraftDocument3 pagesAmbulance Response Protocol DraftCommand CenterNo ratings yet
- Brain TumorsDocument19 pagesBrain TumorsMehjabin mohammedNo ratings yet
- Prepared by Inzar Yasin Ammar LabibDocument47 pagesPrepared by Inzar Yasin Ammar LabibJohn Clements Galiza100% (1)
- Xu Xiangcai - Complete External Therapies of Chinese Drugs PDFDocument555 pagesXu Xiangcai - Complete External Therapies of Chinese Drugs PDFaryaa2020100% (9)
- GI BleedingDocument37 pagesGI BleedingAnamul MasumNo ratings yet
- Hemorrhoids: Ginesha Hafidzy GarishahDocument35 pagesHemorrhoids: Ginesha Hafidzy GarishahrizqinadiaNo ratings yet
- HemorrhageDocument239 pagesHemorrhageparmeshori100% (1)
- HemerroidDocument24 pagesHemerroidVina WineNo ratings yet
- HemorrhoidDocument12 pagesHemorrhoidSasqia Trizolla0% (1)
- Ugib &lgibDocument41 pagesUgib &lgibDawex IsraelNo ratings yet
- Gastro Week 4Document39 pagesGastro Week 4Reynaldi FernandesNo ratings yet
- GI Bleeding 20-21Document38 pagesGI Bleeding 20-212859bathinaNo ratings yet
- HemorrhoidDocument12 pagesHemorrhoidAdelia Maharani DNo ratings yet
- Hemorrhoid Externa: Qara Syifa Fachrani 1610211039Document25 pagesHemorrhoid Externa: Qara Syifa Fachrani 1610211039Qara Syifa FNo ratings yet
- Laporan Kasus - HemorrhoidsDocument41 pagesLaporan Kasus - HemorrhoidsMetyana CahyaningtyasNo ratings yet
- Lower GIT BleedingDocument30 pagesLower GIT BleedingRonald Joy DatuNo ratings yet
- Overview of Lower GastroIntestinal Bleeding 1.1Document42 pagesOverview of Lower GastroIntestinal Bleeding 1.1Raja Ain100% (1)
- Upper Gastrointestinal BleedingDocument46 pagesUpper Gastrointestinal BleedingRashed ShatnawiNo ratings yet
- Pgi Hemorrhoids PresentationDocument41 pagesPgi Hemorrhoids PresentationIkea BalhonNo ratings yet
- Upper GI Bleeding & It's ManagementDocument40 pagesUpper GI Bleeding & It's ManagementManeesha KhalseNo ratings yet
- PR BleedDocument20 pagesPR BleedCathy KayNo ratings yet
- Lower Gastrointestinal Bleeding: Clinical Science SessionDocument48 pagesLower Gastrointestinal Bleeding: Clinical Science SessionNissaa IslamiatiNo ratings yet
- Upper Gastrointestinal BleedingDocument49 pagesUpper Gastrointestinal BleedingUmar AzlanNo ratings yet
- Approach To A Patient With Upper GI BleedDocument42 pagesApproach To A Patient With Upper GI BleedMuhammad Naveed AslamNo ratings yet
- Atul Sharma Uppergi Fcccm23Document47 pagesAtul Sharma Uppergi Fcccm23Atul SharmaNo ratings yet
- What Are The Surgical Complications of Typhoid OrganismDocument15 pagesWhat Are The Surgical Complications of Typhoid OrganismNdenwaneku OkuwaNo ratings yet
- Hemorrhoids: What Are Hemorrhoids? What Are The Symptoms of Hemorrhoids?Document6 pagesHemorrhoids: What Are Hemorrhoids? What Are The Symptoms of Hemorrhoids?Devina NugrohoNo ratings yet
- Topic:Hemorrhoids: Faculty:Ayub Khan Presentation By:group: A Group Leader: Sibghatullah Group MembersDocument21 pagesTopic:Hemorrhoids: Faculty:Ayub Khan Presentation By:group: A Group Leader: Sibghatullah Group MembersYogesh maharajNo ratings yet
- Presented by Mr. Vinay Kumar M.Sc. Nursing 1 Year HCN, SrhuDocument66 pagesPresented by Mr. Vinay Kumar M.Sc. Nursing 1 Year HCN, SrhuVinay Kumar100% (2)
- 3.2 Hematemesis LsyDocument23 pages3.2 Hematemesis Lsymirabel IvanaliNo ratings yet
- UGIBDocument5 pagesUGIBdwyane0033100% (1)
- 3.3 Hematochezia LsyDocument21 pages3.3 Hematochezia Lsymirabel IvanaliNo ratings yet
- Chole CystitisDocument43 pagesChole CystitisBheru LalNo ratings yet
- Clinical Clerk Seminar Series: Approach To Gi BleedsDocument11 pagesClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388No ratings yet
- Course - Subject-Unit / Topic - Title - Prepared byDocument39 pagesCourse - Subject-Unit / Topic - Title - Prepared byEsha KuttiNo ratings yet
- Haemorrhage and ShockDocument112 pagesHaemorrhage and Shocksaranya amuNo ratings yet
- Pemicu 5 GIT DevinDocument131 pagesPemicu 5 GIT DevinDevin AlexanderNo ratings yet
- Notes HemorrhoidsDocument4 pagesNotes HemorrhoidsSanthu Su100% (1)
- HEMORRHOIDSDocument4 pagesHEMORRHOIDSarshi khanNo ratings yet
- Acute GI BleedingDocument35 pagesAcute GI BleedingGalih GimastiarNo ratings yet
- Polyp DKKDocument45 pagesPolyp DKKNadya Beatrix Yohanna NapitupuluNo ratings yet
- K11 Bedah EsofagusDocument37 pagesK11 Bedah EsofagusenriNo ratings yet
- What Are The Signs of Bleeding in The Digestive Tract?Document6 pagesWhat Are The Signs of Bleeding in The Digestive Tract?draganNo ratings yet
- 3Document5 pages3snrarasatiNo ratings yet
- Upper GI Bleed - SymposiumDocument38 pagesUpper GI Bleed - SymposiumSopna ZenithNo ratings yet
- Acute Gi Bleeding: Rohman AzzamDocument34 pagesAcute Gi Bleeding: Rohman AzzamgebyarayuNo ratings yet
- Diagnosis of Gastrointestinal Bleeding: Liu ZhenhuaDocument55 pagesDiagnosis of Gastrointestinal Bleeding: Liu ZhenhuaVitry ErwadiNo ratings yet
- Acute AbdomenDocument24 pagesAcute AbdomenGrace SimmonsNo ratings yet
- The Stomach and Duodenum: Dr. Elian EliasDocument48 pagesThe Stomach and Duodenum: Dr. Elian EliasmodarNo ratings yet
- HemorrhoidsDocument9 pagesHemorrhoidsaix_santosNo ratings yet
- Hemoroid JurnalDocument7 pagesHemoroid JurnalAsti HaryaniNo ratings yet
- Process Plant Layout - Seán Moran 3-4Document2 pagesProcess Plant Layout - Seán Moran 3-4CunCunAlAndraNo ratings yet
- Management Gathering 0718 - Distribution - v5 CoverDocument1 pageManagement Gathering 0718 - Distribution - v5 CoverCunCunAlAndraNo ratings yet
- GF Signet 515 2536 Manual01Document1 pageGF Signet 515 2536 Manual01CunCunAlAndraNo ratings yet
- DA38 Safety Data Shett FAME (Fatty Acid Methyl Ester) V4 - en - DEDocument14 pagesDA38 Safety Data Shett FAME (Fatty Acid Methyl Ester) V4 - en - DECunCunAlAndraNo ratings yet
- Early Liver TransplantationDocument11 pagesEarly Liver TransplantationCunCunAlAndraNo ratings yet
- Problem 5 Git: Ivan MichaelDocument68 pagesProblem 5 Git: Ivan MichaelCunCunAlAndraNo ratings yet
- Pitri - GI.Pemicu 4. GE+ Tifus AbdominalisDocument154 pagesPitri - GI.Pemicu 4. GE+ Tifus AbdominalisCunCunAlAndraNo ratings yet
- Breather Valve - Pressure-Vaccuem Relief ValveDocument2 pagesBreather Valve - Pressure-Vaccuem Relief Valvevphor85No ratings yet
- Tugas Bahasa InggrisDocument3 pagesTugas Bahasa InggrisWendylina BuikNo ratings yet
- Mapeh: Music - Arts - Physical Education - HealthDocument11 pagesMapeh: Music - Arts - Physical Education - HealthKuerth VinluanNo ratings yet
- KIFHP - CARE - First Interim Narrative ReportDocument39 pagesKIFHP - CARE - First Interim Narrative ReportEliNo ratings yet
- An Introduction To The Medical Foods IndustryDocument30 pagesAn Introduction To The Medical Foods IndustryABIOGENDSNo ratings yet
- What Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and UterineDocument18 pagesWhat Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and Uterineمحمداحمد محمدنور ابايزيدNo ratings yet
- Reproductive Health Notes For NEET Download PDF - pdf-24Document4 pagesReproductive Health Notes For NEET Download PDF - pdf-24Sonty100% (1)
- Chapter 14Document42 pagesChapter 14Fatma Taha MohamedNo ratings yet
- Opioides y ArtroplastiaDocument10 pagesOpioides y ArtroplastiaCirugia HEAVNo ratings yet
- Radiology Elective Care HandbookDocument44 pagesRadiology Elective Care HandbookDsk Ricafrente BonitNo ratings yet
- Article À CritiquerDocument10 pagesArticle À CritiquerAs MaaNo ratings yet
- Management of Scabies PDFDocument5 pagesManagement of Scabies PDFAfnindyas AtikaNo ratings yet
- Short GuidelinesDocument52 pagesShort GuidelinesMohamed FaizalNo ratings yet
- Careworld Philippines Inc.: 3 Floor, Amore BLDG., Brgy. Luciano Trecemartires City, Cavite, PhilippinesDocument6 pagesCareworld Philippines Inc.: 3 Floor, Amore BLDG., Brgy. Luciano Trecemartires City, Cavite, PhilippinesRowena Lalongisip De LeonNo ratings yet
- Biology Investigatory ProjectDocument14 pagesBiology Investigatory Projectdesaipiyush1234No ratings yet
- CHORIOAMNIONITISDocument32 pagesCHORIOAMNIONITISnurul azareeNo ratings yet
- National Mental Health Programme, IndiaDocument27 pagesNational Mental Health Programme, Indiadrguptavivek1978No ratings yet
- Waiters Postpartal Hemorrhage PDFDocument1 pageWaiters Postpartal Hemorrhage PDFmp1757No ratings yet
- List of References For Assessment of Hamamelis Virginiana L.Document8 pagesList of References For Assessment of Hamamelis Virginiana L.Miroslav IlicNo ratings yet
- Antenatal Education For First Time MothersDocument26 pagesAntenatal Education For First Time MothersPratik Ranjan NayakNo ratings yet
- Challenging Concepts Book Series OUPDocument11 pagesChallenging Concepts Book Series OUPmakmgmNo ratings yet
- Pulmonary ThrombosisDocument4 pagesPulmonary ThrombosisMafe HerreraNo ratings yet
- 1992 - Kaplan - Blood Pressure Measurement and MonitoringDocument33 pages1992 - Kaplan - Blood Pressure Measurement and MonitoringKTKL RSABNo ratings yet
- Knowledge and Awareness of Traffic Rules and The Impact of Traffic Exposure On College StudentsDocument21 pagesKnowledge and Awareness of Traffic Rules and The Impact of Traffic Exposure On College StudentsQuartey NiiNo ratings yet
- I. Enrichment Activity A. AssessmentDocument3 pagesI. Enrichment Activity A. AssessmentJeko Betguen PalangiNo ratings yet
- 10 - "Crown-then-Graft" - A Novel Approach To OptimizeDocument14 pages10 - "Crown-then-Graft" - A Novel Approach To OptimizePablo BenitezNo ratings yet