You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Dermatologic EmergencyDocument28 pagesDermatologic EmergencyQonita HanifNo ratings yet
- Baldwin Thayer HemifacialSpasm 08 PDFDocument28 pagesBaldwin Thayer HemifacialSpasm 08 PDFQonita HanifNo ratings yet
- PDF JTN 679 PDFDocument7 pagesPDF JTN 679 PDFQonita HanifNo ratings yet
- Nutrisi Dan Gizi BurukDocument9 pagesNutrisi Dan Gizi BurukFifin HestiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Urethral Stricture Diagnosis and TreatmentDocument9 pagesUrethral Stricture Diagnosis and TreatmentNadila Ayu PutriNo ratings yet
- Meagan Blevins ResumeDocument2 pagesMeagan Blevins Resumeapi-549554682No ratings yet
- Conference/Symposium Evaluation Form: 1 Poor 2 Below Average 3 Average 4 Above Average 5 OutstandingDocument2 pagesConference/Symposium Evaluation Form: 1 Poor 2 Below Average 3 Average 4 Above Average 5 Outstandingyos_peace86No ratings yet
- Indian Advanced Wound Care MarketDocument12 pagesIndian Advanced Wound Care MarketManish RastogiNo ratings yet
- Book IndentDocument6 pagesBook Indentpushpajachar95No ratings yet
- Acromegaly Feb2020Document4 pagesAcromegaly Feb2020anlekgenNo ratings yet
- Gudagat Vikar Visheshank July 2009Document8 pagesGudagat Vikar Visheshank July 2009Bharath SHNo ratings yet
- Dr. Richard Teo Gave Inspiring SpeechDocument6 pagesDr. Richard Teo Gave Inspiring Speechpeli1974No ratings yet
- Métodos de Reabilitação para Redução Da Subluxação Do Ombro Na Hemiparesia pós-AVC Uma Revisão SistemátDocument15 pagesMétodos de Reabilitação para Redução Da Subluxação Do Ombro Na Hemiparesia pós-AVC Uma Revisão SistemátMatheus AlmeidaNo ratings yet
- Chapter 1 Introduction To Emergency Medical CareDocument19 pagesChapter 1 Introduction To Emergency Medical Carejmmos207064100% (1)
- Effect of Nateglinide On The Incidence of DiabetesDocument31 pagesEffect of Nateglinide On The Incidence of Diabetesfred opinionNo ratings yet
- OET Corrected Letter 1 - 30 PDFDocument48 pagesOET Corrected Letter 1 - 30 PDFAleyna Shrestha86% (43)
- May 20151Document17 pagesMay 20151Hany Rasheed Mohamed50% (2)
- Association Between Mir Let-7g Gene Expression and The Risk of Cervical Cancer in Human Papilloma Virus-Infected PatientsDocument8 pagesAssociation Between Mir Let-7g Gene Expression and The Risk of Cervical Cancer in Human Papilloma Virus-Infected PatientsGICELANo ratings yet
- Congestive Heart Failure 1 Concept Map !Document1 pageCongestive Heart Failure 1 Concept Map !Franklin A. Salaum IIINo ratings yet
- Rehabilitasi Pasca CABGDocument23 pagesRehabilitasi Pasca CABGPaulina WowilingNo ratings yet
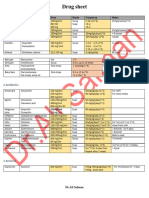
- Pediatrics Drugs-1Document3 pagesPediatrics Drugs-1seemahasheesh93No ratings yet
- Template of Japan RMP-wordDocument14 pagesTemplate of Japan RMP-wordDina AndiniNo ratings yet
- EnucleationDocument6 pagesEnucleationRameez SarwarNo ratings yet
- Dr. Tariq Mahmood Sheikh GP-Diploma MRT (ONCOLOGY)Document3 pagesDr. Tariq Mahmood Sheikh GP-Diploma MRT (ONCOLOGY)cdeekyNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormCyberpoint Internet Cafe and Computer ShopNo ratings yet
- Comparison of The Glimepiride Brand Name Medication and Generic Medications in The Simple Suspension Method and Their Dissolution BehaviorDocument8 pagesComparison of The Glimepiride Brand Name Medication and Generic Medications in The Simple Suspension Method and Their Dissolution BehaviorMohammad BakrNo ratings yet
- The Role of Hospital and Community Pharmacists inDocument15 pagesThe Role of Hospital and Community Pharmacists inMD. NAYMUR RAHMANNo ratings yet
- AYUSH: An Introduction to India's Traditional Medicine SystemsDocument36 pagesAYUSH: An Introduction to India's Traditional Medicine SystemsSadhu PriyankaNo ratings yet
- Pharmaceutical Development WorkshopDocument57 pagesPharmaceutical Development WorkshophuynhvinhquangNo ratings yet
- Vasopressors and Inotropes in Shock ManagementDocument63 pagesVasopressors and Inotropes in Shock ManagementCraig DuHaney50% (2)
- Applied Physics (Project)Document7 pagesApplied Physics (Project)Muhammad AliNo ratings yet
- Yellow Book CDC 2018Document705 pagesYellow Book CDC 2018Johanna Melisa JourdanNo ratings yet
- Diagnosis of Pancreatitis in Dogs and Cats: ReviewDocument14 pagesDiagnosis of Pancreatitis in Dogs and Cats: ReviewMiruna ChiriacNo ratings yet
- Artikel Intubasi Sadar Fiberoptik - RevisiDocument10 pagesArtikel Intubasi Sadar Fiberoptik - RevisiNaufal BinseffNo ratings yet