You might also like
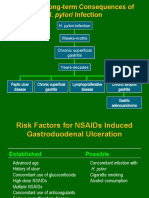
- H. Pylori Infection: Potential Long-Term Consequences ofDocument30 pagesH. Pylori Infection: Potential Long-Term Consequences ofAndrie WigunaNo ratings yet
- Tukak GasterDocument11 pagesTukak GasterAndrie WigunaNo ratings yet
- Helicobacter Pylori: Dr.B.BoyleDocument35 pagesHelicobacter Pylori: Dr.B.BoyleTammy AdjaNo ratings yet
- Pepti C Ul Cer Dis Ea SeDocument36 pagesPepti C Ul Cer Dis Ea Segerald_ichigoNo ratings yet
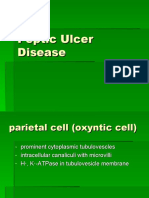
- Peptic Ulcer DiseaseDocument36 pagesPeptic Ulcer DiseasenkpthapanNo ratings yet
- 4. Digestion GM Eng 2020Document49 pages4. Digestion GM Eng 2020snowrose2609No ratings yet
- (Such As Digestive Enzymes, Acid and Bile) : How The Stomach and Intestine Avaoid BeeingDocument27 pages(Such As Digestive Enzymes, Acid and Bile) : How The Stomach and Intestine Avaoid BeeingamalNo ratings yet
- Division of Tropical Medicine and Infectious Diseases at Gatot Soebroto Central Army HospitalDocument63 pagesDivision of Tropical Medicine and Infectious Diseases at Gatot Soebroto Central Army HospitalAggiFitiyaningsihNo ratings yet
- Gastritis: Palangka Raya University Faculty of MedicineDocument32 pagesGastritis: Palangka Raya University Faculty of MedicineAnonymNo ratings yet
- Gastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDDocument82 pagesGastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDAvi Themessy100% (1)
- Peptic Ulcer DiseaseDocument119 pagesPeptic Ulcer DiseaseJoy LacunaNo ratings yet
- Peptic Ulcer and GERD: Chiao-Hsiung ChuangDocument58 pagesPeptic Ulcer and GERD: Chiao-Hsiung ChuangMK CameraNo ratings yet
- Lect - Peptic Ulcer - 211020 - 182113Document38 pagesLect - Peptic Ulcer - 211020 - 182113Puranjay ChandelNo ratings yet
- Stomach PathologyDocument45 pagesStomach PathologytahaNo ratings yet
- Pi Is 0016508597800108Document7 pagesPi Is 0016508597800108Aswani V RaghavanNo ratings yet
- Case 1 - The Heavy Drinker: Faculty of Medicine Mansoura UniversityDocument2 pagesCase 1 - The Heavy Drinker: Faculty of Medicine Mansoura UniversityMuhammar Amin Abd YasinNo ratings yet
- Gastric PathologyDocument11 pagesGastric PathologyAndra BauerNo ratings yet
- Streptococci: S. Pyogenes S. AgalactiaeDocument9 pagesStreptococci: S. Pyogenes S. AgalactiaeChristine BuenNo ratings yet
- Microbial Toxins PDFDocument11 pagesMicrobial Toxins PDFAnonymous OPix6Tyk5INo ratings yet
- Peptic Ulcer DiseaseDocument14 pagesPeptic Ulcer DiseasePernel Jose Alam MicuboNo ratings yet
- PIEPIEDocument23 pagesPIEPIEJaycee NodadoNo ratings yet
- Is Mold Toxicity Really A Problem For Our Patients? Part 2-Nonrespiratory ConditionsDocument7 pagesIs Mold Toxicity Really A Problem For Our Patients? Part 2-Nonrespiratory ConditionsMuhammad Salah AliNo ratings yet
- Hormones and The Gut BjaDocument11 pagesHormones and The Gut BjaAbdulmajeed alluqmaniNo ratings yet
- Immunology & Serology ReviewDocument4 pagesImmunology & Serology Reviewmaria email86% (7)
- 10-Anti Ulcer H2-14-08-2023Document60 pages10-Anti Ulcer H2-14-08-2023ashwin kNo ratings yet
- Bacterial PathogenesisDocument36 pagesBacterial Pathogenesisapi-19969058100% (3)
- Chart - GI InfectionsDocument3 pagesChart - GI InfectionsRedNo ratings yet
- 01 - DiarrheaDocument36 pages01 - DiarrheafrizkapfNo ratings yet
- Campylobacteriosis: A Pediatric Foodborne IllnessDocument18 pagesCampylobacteriosis: A Pediatric Foodborne IllnessRavi PrakashNo ratings yet
- Staphylococcus & StreptococcusDocument100 pagesStaphylococcus & StreptococcusFahim NadvyNo ratings yet
- Gastrointestinal System (Paper-V) PBQs 2018 KU With SolutionsDocument6 pagesGastrointestinal System (Paper-V) PBQs 2018 KU With SolutionsCatalyst NepalNo ratings yet
- (GI) A Child With DiarrheaDocument59 pages(GI) A Child With DiarrheaJo casNo ratings yet
- Pathogenesis and Pathology of Bovine Pne PDFDocument24 pagesPathogenesis and Pathology of Bovine Pne PDFKaran VetNo ratings yet
- S. Aureus, Cons: S.Epidermidis, Cons: S.SaprophyticusDocument14 pagesS. Aureus, Cons: S.Epidermidis, Cons: S.SaprophyticusMugiNo ratings yet
- GastritisDocument3 pagesGastritisaliceNo ratings yet
- Systemic BacteriologyDocument495 pagesSystemic BacteriologyAkash KaranwalNo ratings yet
- Final Interpretation of Endoscopic Gastrointestinal BiopsyDocument107 pagesFinal Interpretation of Endoscopic Gastrointestinal BiopsyyourinmyheartNo ratings yet
- Diseases of The StomachDocument81 pagesDiseases of The StomachIsmail BayraktaroğluNo ratings yet
- Abdomen OSCE (Keys)Document13 pagesAbdomen OSCE (Keys)Saran KumarNo ratings yet
- Normal Flora of The Human BodyDocument37 pagesNormal Flora of The Human Bodyshahbaz100% (6)
- Report On Etiological Structure and Epidemiology of The Acute Intestinal Infections. Pa Tho Genesis of Diarrohea Caused by Infectious Agents.Document3 pagesReport On Etiological Structure and Epidemiology of The Acute Intestinal Infections. Pa Tho Genesis of Diarrohea Caused by Infectious Agents.Adnan Akram, MD (Latvia)No ratings yet
- Normal Flora of The Human BodyDocument38 pagesNormal Flora of The Human BodyTim IT Poltekkes BandungNo ratings yet
- Helicobacter pylori Risk Factors and Clinical ManifestationsDocument2 pagesHelicobacter pylori Risk Factors and Clinical ManifestationsNeil AlviarNo ratings yet
- Immunosero ReviwerDocument73 pagesImmunosero ReviwerDarla YsavelNo ratings yet
- Gastro 2006Document66 pagesGastro 2006Nyoman TapayanaNo ratings yet
- Parasite InfectionsDocument45 pagesParasite InfectionsAbdullah AlkharsNo ratings yet
- Swmana 4 Teórico Digestive DisordersDocument43 pagesSwmana 4 Teórico Digestive DisordersAna Paula Hernández CarballoNo ratings yet
- Dr. GALLEBO's Guide to Histopath and Hepatitis VirusesDocument216 pagesDr. GALLEBO's Guide to Histopath and Hepatitis VirusesFelyne Angelique C. GanoticeNo ratings yet
- GIT OSPE Pathology - Final-2 PDFDocument29 pagesGIT OSPE Pathology - Final-2 PDFafaq alismailiNo ratings yet
- Chapter 21 StaphylococcusDocument40 pagesChapter 21 Staphylococcusyixecix709No ratings yet
- Immunology & Serology Review Notes George Vincent Gellena, RMT, Mls (Ascpi)Document9 pagesImmunology & Serology Review Notes George Vincent Gellena, RMT, Mls (Ascpi)Angelo Jude CobachaNo ratings yet
- SGD Peptic Ulcer DiseaseDocument28 pagesSGD Peptic Ulcer Disease365 DaysNo ratings yet
- Acute Pancreatitis Guide: Causes, Symptoms, TreatmentDocument100 pagesAcute Pancreatitis Guide: Causes, Symptoms, TreatmentabelNo ratings yet
- DiarrheaDocument10 pagesDiarrheaDwi putri PermatasariNo ratings yet
- Kolitis UlseratifDocument6 pagesKolitis UlseratifnurNo ratings yet
- Medical Microbiology: Microbial Toxins & CholeraDocument40 pagesMedical Microbiology: Microbial Toxins & CholerajaymecargnoniNo ratings yet
- 4 Inmunidad InnataDocument40 pages4 Inmunidad InnataLuan NettoNo ratings yet
- Streptococci: Dr. NG Woei KeanDocument30 pagesStreptococci: Dr. NG Woei KeanWong ShuanNo ratings yet
- Interpretation of Gastric BiopsyDocument77 pagesInterpretation of Gastric Biopsyyourinmyheart100% (2)
- ANEMIA Pada Penyakit KronikDocument14 pagesANEMIA Pada Penyakit KronikAndrie WigunaNo ratings yet
- 2014 AHA/ACC Guideline for NSTE-ACS ManagementDocument151 pages2014 AHA/ACC Guideline for NSTE-ACS ManagementParadina WulandariNo ratings yet
- Portaliver USGDocument20 pagesPortaliver USGAndrie WigunaNo ratings yet
- Tukak LambungDocument21 pagesTukak LambungAndrie WigunaNo ratings yet
- HIV Primary Care + Dislipidemia PDFDocument31 pagesHIV Primary Care + Dislipidemia PDFAndrie WigunaNo ratings yet
- Rheumatic Heart Disease MM 06Document9 pagesRheumatic Heart Disease MM 06Оксана МакагоноваNo ratings yet
- 2014 - Acute Rheumatic Fever and Streptococci - The Quintessential Pathogenic Trigger of AutoimmunityDocument10 pages2014 - Acute Rheumatic Fever and Streptococci - The Quintessential Pathogenic Trigger of AutoimmunityAndrie WigunaNo ratings yet
- HEART FAILURE-WilliamDec (2005) PDFDocument602 pagesHEART FAILURE-WilliamDec (2005) PDFChintya Fidelia MontangNo ratings yet
- Hershman2018 PDFDocument10 pagesHershman2018 PDFAndrie WigunaNo ratings yet
- Obesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Document27 pagesObesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Andrie WigunaNo ratings yet
- Acinetobacter BoumaniiDocument8 pagesAcinetobacter BoumaniiAndrie WigunaNo ratings yet
- Pneumonia EpidemiologyDocument18 pagesPneumonia EpidemiologyAndrie WigunaNo ratings yet
- Ultrasound (Kidney)Document28 pagesUltrasound (Kidney)Andrie WigunaNo ratings yet
- 303 - Pathogenic Mechanisms in Rheumatic Carditis - Focus On Valvular EndotheliumDocument5 pages303 - Pathogenic Mechanisms in Rheumatic Carditis - Focus On Valvular EndotheliumAndrie WigunaNo ratings yet
- Efek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularDocument6 pagesEfek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularAndrie WigunaNo ratings yet
- 1989 - Streptococcal M Protein-Design and Biological Bahaviour PDFDocument30 pages1989 - Streptococcal M Protein-Design and Biological Bahaviour PDFAndrie WigunaNo ratings yet
- PRESENTASI KASUS SirosisDocument11 pagesPRESENTASI KASUS SirosisAndrie WigunaNo ratings yet
- Antiplateletdrugs 150203231404 Conversion Gate01 PDFDocument67 pagesAntiplateletdrugs 150203231404 Conversion Gate01 PDFAndrie WigunaNo ratings yet
- PAD Guideline AHA-ACC 2016Document23 pagesPAD Guideline AHA-ACC 2016Andrie WigunaNo ratings yet
- Hershman2018 PDFDocument10 pagesHershman2018 PDFAndrie WigunaNo ratings yet
- Case Malaria YosuiDocument56 pagesCase Malaria YosuiAndrie WigunaNo ratings yet
- Antiplateletdrugs 150203231404 Conversion Gate01 PDFDocument67 pagesAntiplateletdrugs 150203231404 Conversion Gate01 PDFAndrie WigunaNo ratings yet
- Gambar DigestiveDocument1 pageGambar DigestiveAndrie WigunaNo ratings yet
- Nosocomial Pneumonia in AdultsDocument28 pagesNosocomial Pneumonia in AdultsAndrie WigunaNo ratings yet
- Prosedur PCRDocument26 pagesProsedur PCRDevi Widyaningrum100% (1)
- Absence of An Effect of Liposuction On Insulin Action and Risk Factors For Coronary Heart DiseaseDocument14 pagesAbsence of An Effect of Liposuction On Insulin Action and Risk Factors For Coronary Heart DiseaseAndrie WigunaNo ratings yet
- DIVERTIKULOSISDocument28 pagesDIVERTIKULOSISAndrie WigunaNo ratings yet
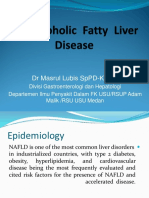
- NAFLD-dr. Masrul KuliahDocument103 pagesNAFLD-dr. Masrul KuliahAndrie WigunaNo ratings yet
- Among Diabetic Participant in The ILOPE Study Who Did Not Have Microalbuminuria at Base LineDocument1 pageAmong Diabetic Participant in The ILOPE Study Who Did Not Have Microalbuminuria at Base LineAndrie WigunaNo ratings yet
- Combining Singing and PsycologyDocument6 pagesCombining Singing and PsycologyAna luciaNo ratings yet
- Sharp Sharp Cash Register Xe A207 Users Manual 284068Document1 pageSharp Sharp Cash Register Xe A207 Users Manual 284068Zeila CordeiroNo ratings yet
- 1675.does Concrete Lighten or Change Color As It DriesDocument5 pages1675.does Concrete Lighten or Change Color As It DriestvrNo ratings yet
- 1 Catalyst FundamentalsDocument17 pages1 Catalyst FundamentalsSam AnuNo ratings yet
- Living Together TestDocument2 pagesLiving Together TestProfu' de biologieNo ratings yet
- 2011 Mena Annual Reportv1Document73 pages2011 Mena Annual Reportv1Yasmeen LayallieNo ratings yet
- Development PlanningDocument15 pagesDevelopment PlanningSamuelNo ratings yet
- Flavors Supplies BudgetDocument6 pagesFlavors Supplies BudgetJomarie EmilianoNo ratings yet
- GeM Bidding 3702669Document10 pagesGeM Bidding 3702669ANIMESH JAINNo ratings yet
- 5G Antenna Talk TWDocument48 pages5G Antenna Talk TWRohit MathurNo ratings yet
- Families of Carbon Compounds: Functional Groups, Intermolecular Forces, & Infrared (IR) SpectrosDocument79 pagesFamilies of Carbon Compounds: Functional Groups, Intermolecular Forces, & Infrared (IR) SpectrosRuryKharismaMuzaqieNo ratings yet
- 2nd Chapter Notes Mechanical Engineering DiplomaDocument7 pages2nd Chapter Notes Mechanical Engineering DiplomaUsmanNo ratings yet
- Automation of Banking Service - EBL & EXIM BankDocument32 pagesAutomation of Banking Service - EBL & EXIM BankShaffyNo ratings yet
- The Impact of Spiritual Intelligence, Gender and Educational Background On Mental Health Among College StudentsDocument22 pagesThe Impact of Spiritual Intelligence, Gender and Educational Background On Mental Health Among College StudentsBabar MairajNo ratings yet
- Carbon Disulfide: Hazard SummaryDocument5 pagesCarbon Disulfide: Hazard SummaryAlyssa ZerlinaNo ratings yet
- Ethylene Yield From Pyrolysis Cracking in Olefin PDocument6 pagesEthylene Yield From Pyrolysis Cracking in Olefin PALL2WINNo ratings yet
- 10 - (Rahman) The Relationship Between Chest Tube Size and Clinical Outcome in Pleural InfectionDocument8 pages10 - (Rahman) The Relationship Between Chest Tube Size and Clinical Outcome in Pleural InfectionfaisaldanyaniNo ratings yet
- Acrogym: by Ahana AnandDocument9 pagesAcrogym: by Ahana AnandAhana AnandNo ratings yet
- Carbon Emission and Battery Monitoring SystemDocument17 pagesCarbon Emission and Battery Monitoring SystemIJRASETPublicationsNo ratings yet
- ĐỀ THI HSGDocument13 pagesĐỀ THI HSGahmad amdaNo ratings yet
- OlayDocument36 pagesOlayrachit.chaudharyNo ratings yet
- Overview of Research ProcessDocument31 pagesOverview of Research Processprema balusamyNo ratings yet
- Eshe July-Aug 2021Document56 pagesEshe July-Aug 2021eSheNo ratings yet
- Exam Unit 1 Out and About 1º BachilleratoDocument5 pagesExam Unit 1 Out and About 1º Bachilleratolisikratis1980No ratings yet
- The Greatest Showman PDFDocument22 pagesThe Greatest Showman PDFMJ RecordNo ratings yet
- Chakra System of Animals FACT SHEETDocument4 pagesChakra System of Animals FACT SHEETNiko Diamesis75% (4)
- Bomba de Vacio Part ListDocument2 pagesBomba de Vacio Part ListNayeli Zarate MNo ratings yet
- Summary G.E 9 Rizal Works (Chapter 1-13)Document23 pagesSummary G.E 9 Rizal Works (Chapter 1-13)Erwin Jay CabantacNo ratings yet
- ADWEA Approved Vendor List - 18.4.2013Document297 pagesADWEA Approved Vendor List - 18.4.2013Anonymous kjvaeVJNNo ratings yet
- Battle Bikes 2.4 PDFDocument56 pagesBattle Bikes 2.4 PDFfranzyland100% (1)