You might also like
- Meltdown at 3 Mile Island: Akshit Arora (201) Yash BhayaniDocument15 pagesMeltdown at 3 Mile Island: Akshit Arora (201) Yash BhayaniAkshit AroraNo ratings yet
- Tmi NotesDocument2 pagesTmi Notesgeorge aarthiNo ratings yet
- Three Mile Island Nuclear Accident of 1979Document22 pagesThree Mile Island Nuclear Accident of 1979VP Ch4nelNo ratings yet
- Nuclear Reactor Meltdown: The Three Mile Island AccidentDocument23 pagesNuclear Reactor Meltdown: The Three Mile Island AccidentZim VicomNo ratings yet
- AccidentsDocument9 pagesAccidentsAmeer HussainNo ratings yet
- Three Mile Island AccidentDocument8 pagesThree Mile Island AccidentJeyakrishnan CNo ratings yet
- Hotwell Overflow Causes Boiler Tube MeltdownDocument4 pagesHotwell Overflow Causes Boiler Tube MeltdownakarshansoodNo ratings yet
- Three Mile Island AccidentDocument18 pagesThree Mile Island Accidentsoha89No ratings yet
- The TMI-2 Accident - in BriefDocument2 pagesThe TMI-2 Accident - in BriefMuhammad RehanNo ratings yet
- Three Mile IslandDocument5 pagesThree Mile IslandJulian Ee Zhi HowNo ratings yet
- Operation & Maintenance Manual: For Khartoum North Power Station-Phase Iii (2×100Mw) ProjectDocument7 pagesOperation & Maintenance Manual: For Khartoum North Power Station-Phase Iii (2×100Mw) ProjectVivek SakthiNo ratings yet
- 1 - LAGEN - Chapitre 7Document52 pages1 - LAGEN - Chapitre 7Ajrod RodNo ratings yet
- Formosa PVC ExplosionDocument11 pagesFormosa PVC ExplosionNatasha OliviaNo ratings yet
- English Manual PDFDocument16 pagesEnglish Manual PDFARISNo ratings yet
- YB Lucky Cement Limited: Work InstructionDocument9 pagesYB Lucky Cement Limited: Work Instructionshani5573No ratings yet
- Fukushima Event PCTRAN AnalysisDr LI-Chi Cliff PoDocument16 pagesFukushima Event PCTRAN AnalysisDr LI-Chi Cliff PoEnformableNo ratings yet
- Part 4 Thermal Cycle and Turbine Aux.: Chapter DescriptionDocument27 pagesPart 4 Thermal Cycle and Turbine Aux.: Chapter Descriptionkeerthi dayarathnaNo ratings yet
- Ai Boiler Routine Maintenance Guide: AmerecDocument10 pagesAi Boiler Routine Maintenance Guide: Amerecأبو نبيل سلامNo ratings yet
- IPCDocument2 pagesIPCjeeldhameliya82No ratings yet
- Power Plant EmergeneciesDocument30 pagesPower Plant Emergeneciesrnumesh1100% (1)
- 3.SOP of Pretreatment PlantDocument4 pages3.SOP of Pretreatment PlantBARNALI MUKHERJEE100% (1)
- CANDU reactors use multiple safety systems to safely shut down and contain radiationDocument2 pagesCANDU reactors use multiple safety systems to safely shut down and contain radiationEN IDNo ratings yet
- Technical Briefing: Javier YlleraDocument9 pagesTechnical Briefing: Javier YlleraDeepak BNNo ratings yet
- Multi-Unit Shutdown Due To Boiler Feedwater Chemical ExcursionDocument22 pagesMulti-Unit Shutdown Due To Boiler Feedwater Chemical ExcursionPatrick ramotlopiNo ratings yet
- Pump and Motor Failure in A Hot Potassium-Carbonate SystemAiche-1981-010Document4 pagesPump and Motor Failure in A Hot Potassium-Carbonate SystemAiche-1981-010Hsein WangNo ratings yet
- Unit 2 AOH Recom. ReportDocument12 pagesUnit 2 AOH Recom. Reportanil peralaNo ratings yet
- APPENDIX 2 Occupational Radiation Dose Distribution at Loviisa and Olkiluoto Nuclear Power Plants in 2012Document30 pagesAPPENDIX 2 Occupational Radiation Dose Distribution at Loviisa and Olkiluoto Nuclear Power Plants in 2012LoffeguttNo ratings yet
- The Hydrocracker Explosion and Fire: MarchDocument21 pagesThe Hydrocracker Explosion and Fire: MarchMoca PhoenixNo ratings yet
- Chernobyl Disaster: Saurabh Bhavsar Ameya Borwankar Akshay Chaubal Rohan ChaukulkarDocument17 pagesChernobyl Disaster: Saurabh Bhavsar Ameya Borwankar Akshay Chaubal Rohan ChaukulkarRamu KrishnanNo ratings yet
- Wood Creek International School ReportDocument5 pagesWood Creek International School ReportEvah AdamsNo ratings yet
- Chernobyl DisasterDocument9 pagesChernobyl DisastervivekvpsfeNo ratings yet
- Hgu - ImergencyDocument15 pagesHgu - Imergencyravi kansagaraNo ratings yet
- Burnout of No.2 Main Inert Gas Fan Motor of Crude-Oil TankerDocument2 pagesBurnout of No.2 Main Inert Gas Fan Motor of Crude-Oil TankerRani NoumanNo ratings yet
- Flare Line Failure Case, What We Have LearnedDocument20 pagesFlare Line Failure Case, What We Have LearnedNABEEL VMNo ratings yet
- Troubleshooting Distillation ColumnsDocument6 pagesTroubleshooting Distillation ColumnsRahul ChandrawarNo ratings yet
- Group 1A - Lab Report Combine PDFDocument87 pagesGroup 1A - Lab Report Combine PDFHanifatur AffiqNo ratings yet
- Nuclear FinalDocument2 pagesNuclear Finalapi-285915181No ratings yet
- Model N18-4.9 (470 ) 18Mw Condensing Steam TurbineDocument20 pagesModel N18-4.9 (470 ) 18Mw Condensing Steam TurbineFajarnurjamanNo ratings yet
- 04 - Turbine Trip (CNK 12 M Ove Oi 204C) +Document7 pages04 - Turbine Trip (CNK 12 M Ove Oi 204C) +Your FriendNo ratings yet
- Urea Plant SopDocument52 pagesUrea Plant SopAnjal DuttaNo ratings yet
- Safety in Chemical EngineeringDocument37 pagesSafety in Chemical EngineeringAbhishek VermaNo ratings yet
- Unexpected Drop of The Reactor PowerDocument5 pagesUnexpected Drop of The Reactor PowerGrayNo ratings yet
- A Safety-Alert-Maintenance 1-IADC PDFDocument2 pagesA Safety-Alert-Maintenance 1-IADC PDFVeeramuthu SundararajuNo ratings yet
- V1-4Document24 pagesV1-4Alexander BaziotisNo ratings yet
- A Safety Alert Maintenance 1 IADCDocument2 pagesA Safety Alert Maintenance 1 IADCvsrslmNo ratings yet
- When Isolations Go Wrong: 5 Case Studies on Isolation FailuresDocument44 pagesWhen Isolations Go Wrong: 5 Case Studies on Isolation FailuresenriqueramoscNo ratings yet
- Grinding Area Problems. Date 26.01.2023Document1 pageGrinding Area Problems. Date 26.01.2023Malla GaneshNo ratings yet
- Overhauling Surprises of Unit # 4: Electrical & C&IDocument4 pagesOverhauling Surprises of Unit # 4: Electrical & C&ISony RamaNo ratings yet
- Report On Potable Water High Temperature Issue Rev-1Document3 pagesReport On Potable Water High Temperature Issue Rev-1tere_naam8812142No ratings yet
- Incident Report PDFDocument2 pagesIncident Report PDFParekh KarNo ratings yet
- Nuclear power plant reactors: Pressurized water and boiling waterDocument35 pagesNuclear power plant reactors: Pressurized water and boiling waterSujay SaxenaNo ratings yet
- Ac Report 02-01-2023Document14 pagesAc Report 02-01-2023BalajiNo ratings yet
- TEPCO's Nuclear Power Plantssuffered From Big Earthquake Ofmarch 11,2011Document22 pagesTEPCO's Nuclear Power Plantssuffered From Big Earthquake Ofmarch 11,2011EnformableNo ratings yet
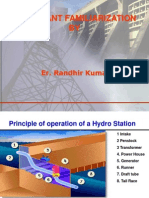
- How hydro power plants generate electricityDocument45 pagesHow hydro power plants generate electricityrandhir1112100% (1)
- Shell and Tube Heat Exchanger User's ManualDocument5 pagesShell and Tube Heat Exchanger User's ManualinstrutechNo ratings yet
- Chemical Cleaning of Boiler Pressure Parts As TheDocument57 pagesChemical Cleaning of Boiler Pressure Parts As TheAnonymous 1OmAQ0u3No ratings yet
- CFBC Refractory Dryout Along With Atmospheric Boilout FinalDocument7 pagesCFBC Refractory Dryout Along With Atmospheric Boilout FinalpurvgargNo ratings yet
- Chemical Process Safety: Learning from Case HistoriesFrom EverandChemical Process Safety: Learning from Case HistoriesRating: 4 out of 5 stars4/5 (14)
- BGyan Newsletter 01Dec-07DecDocument10 pagesBGyan Newsletter 01Dec-07DeckiranradNo ratings yet
- BGyan17 17nov 23novDocument11 pagesBGyan17 17nov 23novkiranradNo ratings yet
- BGyan17 14sept 20septDocument12 pagesBGyan17 14sept 20septkiranradNo ratings yet
- BGyan Newsletter - 24nov - 30novDocument11 pagesBGyan Newsletter - 24nov - 30novkiranradNo ratings yet
- BGyan Newsletter - 20oct - 26 October, 2010Document11 pagesBGyan Newsletter - 20oct - 26 October, 2010kiranradNo ratings yet
- BGyan Newsletter - 27 October - 09 November, 2010Document11 pagesBGyan Newsletter - 27 October - 09 November, 2010kiranradNo ratings yet
- BGyan Newsletter - 10 November - 16 NovemberDocument11 pagesBGyan Newsletter - 10 November - 16 NovemberkiranradNo ratings yet
- BGyan Newsletter - 13oct - 19 Oct, 2010Document11 pagesBGyan Newsletter - 13oct - 19 Oct, 2010kiranradNo ratings yet
- BGyan Newsletter - 06 Oct - 12 Oct, 2010Document11 pagesBGyan Newsletter - 06 Oct - 12 Oct, 2010kiranradNo ratings yet
- BGyan17 29sept 05octDocument11 pagesBGyan17 29sept 05octkiranradNo ratings yet
- PlachimadaDocument19 pagesPlachimadakiranradNo ratings yet
- Foreign Affairs - 2022 September-OctoberDocument272 pagesForeign Affairs - 2022 September-OctoberHaris Riski100% (3)
- Saudi NEOM Nuclear - Saudi NEOM ChinaDocument3 pagesSaudi NEOM Nuclear - Saudi NEOM ChinaArab WatchdogNo ratings yet
- Essay - Impacts of Nuclear Science and TechnologyDocument1 pageEssay - Impacts of Nuclear Science and TechnologyMarvin Villanueva LPTNo ratings yet
- Godzilla To Hit King Kong King Kong To Hit GodzillaDocument10 pagesGodzilla To Hit King Kong King Kong To Hit GodzillaNamelessNo ratings yet
- Criteria For Radionuclide Activity Concentrations For Food and Drinking Water IAEADocument63 pagesCriteria For Radionuclide Activity Concentrations For Food and Drinking Water IAEAabdulaziz saadNo ratings yet
- Development of Envo Law (Nasional & Global)Document26 pagesDevelopment of Envo Law (Nasional & Global)Wahyu Yun SantosoNo ratings yet
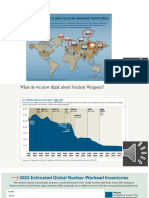
- Lesson+2 +Nuke+Map +Nuclear+Weapons+TodayDocument34 pagesLesson+2 +Nuke+Map +Nuclear+Weapons+Todaykylemistry02No ratings yet
- Process EssayDocument5 pagesProcess EssayNhi QuỳnhNo ratings yet
- Delta Green - Adv - WormwoodDocument8 pagesDelta Green - Adv - WormwoodAirborne PotatoNo ratings yet
- Hibakusha Testimonies BookDocument417 pagesHibakusha Testimonies BookToumany SidibeNo ratings yet
- Devil RunDocument51 pagesDevil RunSergio Jaimez100% (1)
- Environmental Law - Nuclear Energy and LawDocument13 pagesEnvironmental Law - Nuclear Energy and LawMasoom RezaNo ratings yet
- Test 12Document6 pagesTest 12Nguyệt ChiNo ratings yet
- Rakshith H J Pes1202102889 Ble Cs7Document3 pagesRakshith H J Pes1202102889 Ble Cs7Rakshith naiduNo ratings yet
- Position PaperDocument3 pagesPosition PaperAlthea SJNo ratings yet
- Dynamic Response and Failure Analysis of Intze Storage Tanks Under External Blast LoadingDocument163 pagesDynamic Response and Failure Analysis of Intze Storage Tanks Under External Blast LoadingharshNo ratings yet
- Why I Chose the University of Mindanao for Its Affordable Tuition and Convenient Term CalendarDocument2 pagesWhy I Chose the University of Mindanao for Its Affordable Tuition and Convenient Term Calendarofelia guinitaranNo ratings yet
- Three Miles Island 1979Document1 pageThree Miles Island 1979Ahmad PahrinNo ratings yet
- Safety Behaviours: Human Factors For Pilots 2nd Edition: Resource Booklet 2 Safety CultureDocument32 pagesSafety Behaviours: Human Factors For Pilots 2nd Edition: Resource Booklet 2 Safety CultureSonya McSharkNo ratings yet
- VSTEP Listening TestDocument7 pagesVSTEP Listening Testtieen379No ratings yet
- Age factor literacy second language SEODocument6 pagesAge factor literacy second language SEOabdulNo ratings yet
- SURA - The Russia HAARP Which Could Destroy USA in One Fell Swoop - Reality-ChoiceDocument7 pagesSURA - The Russia HAARP Which Could Destroy USA in One Fell Swoop - Reality-Choicehansley cookNo ratings yet
- Nuclear Energy in UgandaDocument9 pagesNuclear Energy in Ugandamotoy asaph musanNo ratings yet
- IAEA Forum on SMR Technology and DeploymentDocument50 pagesIAEA Forum on SMR Technology and DeploymentFikri FurqanNo ratings yet
- Genetic Effects of Chernobyl Radiation: Date: Source: SummaryDocument2 pagesGenetic Effects of Chernobyl Radiation: Date: Source: SummaryFred PascuaNo ratings yet
- Nuclear Proliferation: The Beginning of Nuclear AgeDocument5 pagesNuclear Proliferation: The Beginning of Nuclear AgeSami ullah khan BabarNo ratings yet
- Activity Lesson 1 and 2Document4 pagesActivity Lesson 1 and 2Jho Anne Ronquillo LasicNo ratings yet
- Dark Heresy - Imperial Atomica 1.1Document65 pagesDark Heresy - Imperial Atomica 1.1Radosław Kwieciński100% (1)
- Worksheet 2: Identify The Tenses From The Passage BelowDocument3 pagesWorksheet 2: Identify The Tenses From The Passage BelowRiza AgungNo ratings yet
- PHD Thesis Andre Calado CoroadoDocument166 pagesPHD Thesis Andre Calado CoroadoAndré Calado CoroadoNo ratings yet