You might also like
- Respiration 11 Bronchogenic CarcinomaDocument48 pagesRespiration 11 Bronchogenic Carcinomaapi-19641337No ratings yet
- Lung CancerDocument51 pagesLung Cancercharansri821No ratings yet
- Lung Cancer: by Holly Winn and Cathy Mac DonaldDocument49 pagesLung Cancer: by Holly Winn and Cathy Mac DonaldfajarnugrahamulyaNo ratings yet
- 11 Lung CancerDocument30 pages11 Lung CancerMuhammadNo ratings yet
- Lung Cancer Presentation FinalDocument48 pagesLung Cancer Presentation Finalراس زهد ارفنندNo ratings yet
- Lung CancerDocument57 pagesLung CancerOmar HamwiNo ratings yet
- Lung Cancer: Dr. Bhupendra Kaushik Dr. Deepti Sharma MU-2Document49 pagesLung Cancer: Dr. Bhupendra Kaushik Dr. Deepti Sharma MU-2sharmadeepti1992No ratings yet
- Lung CancerDocument24 pagesLung CancerArshamNo ratings yet
- Lung Cancer Presentation FinalDocument40 pagesLung Cancer Presentation Finaljamestarerakshal7329No ratings yet
- Lung CancerDocument29 pagesLung CancerMierre SiriusNo ratings yet
- Lung Cancer Presentation FinalDocument48 pagesLung Cancer Presentation FinalMarc Andrew100% (3)
- Bronkogenik KarsinomaDocument55 pagesBronkogenik KarsinomaPandu AlanNo ratings yet
- Textbook of MedicineDocument5 pagesTextbook of MedicineSudip DevadasNo ratings yet
- Lung Tumours: Bronchogenic Carcinoma Bronchial Carcinoid and Other Tumours Metastatic TumoursDocument41 pagesLung Tumours: Bronchogenic Carcinoma Bronchial Carcinoid and Other Tumours Metastatic Tumoursvintock1979No ratings yet
- Lung Cancer 2020Document68 pagesLung Cancer 2020ebkai98No ratings yet
- Malignant Liver Tumors Undergrad 6th Year Students SharaanDocument56 pagesMalignant Liver Tumors Undergrad 6th Year Students SharaanMohamed AhmedNo ratings yet
- Urological TumoursDocument68 pagesUrological TumoursDr Anais AsimNo ratings yet
- Oncology Disorders StudentDocument41 pagesOncology Disorders StudentshougNo ratings yet
- Lung CarcinomaDocument29 pagesLung Carcinomavinoedhnaidu_rajagopalNo ratings yet
- Emergency in OncologiDocument70 pagesEmergency in OncologiAzwin KamarNo ratings yet
- Bronchogenic Carcinoma: Dr. Vineet ChauhanDocument49 pagesBronchogenic Carcinoma: Dr. Vineet ChauhanRaviNo ratings yet
- Lung Cancer: By: Faezah Nur Mohd Redzwan Nooratiqah RahmatDocument30 pagesLung Cancer: By: Faezah Nur Mohd Redzwan Nooratiqah RahmatDumora FatmaNo ratings yet
- Presentation Small Cell Lung CancerDocument59 pagesPresentation Small Cell Lung Cancerprudhviraj mNo ratings yet
- Lung CancerDocument7 pagesLung CancerClarinda RondainNo ratings yet
- Oleh: DR - Hans Marpaung, SPB, FicsDocument75 pagesOleh: DR - Hans Marpaung, SPB, FicsIrma Julyanti PanggabeanNo ratings yet
- Report NCM 106Document47 pagesReport NCM 106Fair LeenNo ratings yet
- Renal Parenchymal TumorsDocument45 pagesRenal Parenchymal TumorsDaniel100% (1)
- 2.lung NeoplasmDocument50 pages2.lung Neoplasmtesfayegermame95.tgNo ratings yet
- Lung Cancer UdahDocument20 pagesLung Cancer UdahSivi Budiananda SholikhahNo ratings yet
- Neoplasms of The Genitourinary TractDocument71 pagesNeoplasms of The Genitourinary Tractvishalzenia100% (2)
- DR 180114164748Document43 pagesDR 180114164748Hasnain ToheedNo ratings yet
- BronchoDocument15 pagesBronchoCharleneBunquinNo ratings yet
- Lung CancerDocument8 pagesLung CancerGian Arlo Hilario CastroNo ratings yet
- Tumor UG - Edit 1Document74 pagesTumor UG - Edit 1Krisna Adhitya WilantaraNo ratings yet
- Carcinoma Thyroid: Diagnosis and Management: Professor Ravi KantDocument51 pagesCarcinoma Thyroid: Diagnosis and Management: Professor Ravi KantMubarakDiedaNo ratings yet
- Tumours of Lung 19.3.19Document29 pagesTumours of Lung 19.3.19PradeepNo ratings yet
- Esophageal CADocument56 pagesEsophageal CAEdwin OkonNo ratings yet
- Urology Sub Division Department of Surgery Medical School University of Sumatera UtaraDocument26 pagesUrology Sub Division Department of Surgery Medical School University of Sumatera UtaraAulia SiregarNo ratings yet
- Lung CancerDocument19 pagesLung Cancerj.doe.hex_87No ratings yet
- Solitary Pulmonary Nodule (SPN (Document59 pagesSolitary Pulmonary Nodule (SPN (mahmod omerNo ratings yet
- Hemoptysis: Contribution of The Computed Tomography (CT) : CC CBGDocument23 pagesHemoptysis: Contribution of The Computed Tomography (CT) : CC CBGAnonymous h0DxuJTNo ratings yet
- Urinary Bladder and Renal Cell CarcinomaDocument21 pagesUrinary Bladder and Renal Cell CarcinomaYazeed AsrawiNo ratings yet
- Clinical Pharmacy PPT 1Document44 pagesClinical Pharmacy PPT 1Umair MazharNo ratings yet
- Surgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal GlandsDocument38 pagesSurgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal Glandssorin niky mocanu100% (1)
- Group 8: Parik Rabasto Patel, D Patel, J Raghuwanshi Regis Moleta Moreno NaromalDocument35 pagesGroup 8: Parik Rabasto Patel, D Patel, J Raghuwanshi Regis Moleta Moreno NaromalDominique RabastoNo ratings yet
- Urogenital TumorDocument71 pagesUrogenital TumorJanet UngNo ratings yet
- Primary Lung CancerDocument53 pagesPrimary Lung CancerIsaac MwangiNo ratings yet
- Lung & Mediastinal CancerDocument50 pagesLung & Mediastinal Cancercharlesy T0% (1)
- Practice Essentials: Signs and SymptomsDocument20 pagesPractice Essentials: Signs and SymptomsrainbowshopNo ratings yet
- The Management of Lung Cancer - Prof. AnwarDocument106 pagesThe Management of Lung Cancer - Prof. AnwardewitaNo ratings yet
- Askep CA Paru OkDocument70 pagesAskep CA Paru OkLisa KurniaNo ratings yet
- Guidelines On Testicular Cancer: (Limited Text Update March 2009)Document18 pagesGuidelines On Testicular Cancer: (Limited Text Update March 2009)PJ CoNo ratings yet
- Renal CancerDocument34 pagesRenal CancerArya100% (1)
- Prostate Cancer 111606Document31 pagesProstate Cancer 111606abd12medyNo ratings yet
- Hoffman 2000Document7 pagesHoffman 2000jenny12No ratings yet
- Uterine Cancer Pa Tho PhysiologyDocument17 pagesUterine Cancer Pa Tho PhysiologyJeneva L. Lauzon100% (2)
- CT Applications in Chest PathologyDocument16 pagesCT Applications in Chest PathologyNilanka SandunNo ratings yet
- LUNG CaDocument59 pagesLUNG CaokaciaNo ratings yet
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- Final Obgn HandoutDocument36 pagesFinal Obgn HandoutAhmad Faizul AbdrahmansazliNo ratings yet
- End Round of Dermatology, MCQsDocument20 pagesEnd Round of Dermatology, MCQsMuhdZaeed100% (2)
- Sticky Notes Tips Houseman Compilation 389259Document66 pagesSticky Notes Tips Houseman Compilation 389259MuhdZaeed100% (3)
- MCQ OpthalmologyDocument45 pagesMCQ OpthalmologyMuhdZaeed100% (1)
- Ear Nose ThroatDocument34 pagesEar Nose ThroatMuhdZaeedNo ratings yet
- 4 Year Exam: Test 2Document34 pages4 Year Exam: Test 2MuhdZaeedNo ratings yet
- Ent Practical Examinations Slides For StudyDocument31 pagesEnt Practical Examinations Slides For StudyMuhdZaeedNo ratings yet
- ENTDocument73 pagesENTMuhdZaeedNo ratings yet
- Viral KeratitisDocument11 pagesViral KeratitisMuhdZaeedNo ratings yet
- HistoryDocument15 pagesHistoryDanica Mae PepitoNo ratings yet
- Renal Failure Cronic Group 6Document18 pagesRenal Failure Cronic Group 6Wiwi Hardiyanti100% (1)
- Vital Sign AssessmentDocument48 pagesVital Sign Assessmentapi-271649833No ratings yet
- DDEX37 Herald of The MoonDocument39 pagesDDEX37 Herald of The MoonCarl Max Bobo100% (5)
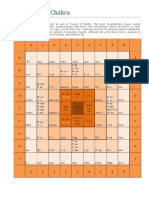
- Sarvatobhadra ChakraDocument6 pagesSarvatobhadra Chakrasateesh_chandra_1100% (5)
- Wa0003Document31 pagesWa0003Anil SinghNo ratings yet
- Jin Shin JyutsuDocument14 pagesJin Shin JyutsuAjay Patil100% (3)
- Pablo de Egina, Medicina 2Document536 pagesPablo de Egina, Medicina 2ataulfNo ratings yet
- 1 4931693113845481676 PDFDocument590 pages1 4931693113845481676 PDFRene Cardozo100% (4)
- Case Report BursitisDocument19 pagesCase Report BursitisFadli Fadil R RNo ratings yet
- Devpsych Reviewer 1Document56 pagesDevpsych Reviewer 1Joshua MalloNo ratings yet
- Toxic Plants in Traditional Indian Systems of Medicine: Thomas M.Walter, Gopi G.RadhaDocument8 pagesToxic Plants in Traditional Indian Systems of Medicine: Thomas M.Walter, Gopi G.Radharajesh_rajesh_rajeshNo ratings yet
- Ranunculacae FamilyDocument39 pagesRanunculacae Familytakne_007No ratings yet
- Review of Systems: Nurs 02 - Health AssessmentDocument22 pagesReview of Systems: Nurs 02 - Health AssessmentteuuuuNo ratings yet
- A Heavy Burden On Young Minds The Global Burden of Mental and Substance Use Disorders in Children and YouthDocument13 pagesA Heavy Burden On Young Minds The Global Burden of Mental and Substance Use Disorders in Children and YouthNatasha AlbaShakiraNo ratings yet
- Gastrointestinal and MetabolismDocument5 pagesGastrointestinal and MetabolismDan HizonNo ratings yet
- Early Onset SchizophreniaDocument3 pagesEarly Onset SchizophreniaDoc Prince CaballeroNo ratings yet
- Anatomy of Stomach and Small IntestineDocument64 pagesAnatomy of Stomach and Small IntestineJessica G. SalimNo ratings yet
- Lymphatic System DiseasesDocument1 pageLymphatic System DiseasesRJ San JuanNo ratings yet
- Spinal Disorders - Study GuideDocument183 pagesSpinal Disorders - Study Guidetechsupport24712365No ratings yet
- Counseling Depressed ElderlyDocument4 pagesCounseling Depressed ElderlyLara Sabunod - PalloNo ratings yet
- Neonatalhypoglycemia: Is There A Sweet Spot?Document14 pagesNeonatalhypoglycemia: Is There A Sweet Spot?karisman kadirNo ratings yet
- PSYCHIATRY Classification of Psychiatric Disorder (Dr. Rosal)Document11 pagesPSYCHIATRY Classification of Psychiatric Disorder (Dr. Rosal)Valcrist BalderNo ratings yet
- What Is Vitamin B12 Good For: Vitamins Vitamin B Niacin Folic Acid Vitamin B12Document75 pagesWhat Is Vitamin B12 Good For: Vitamins Vitamin B Niacin Folic Acid Vitamin B12Nanda SuchirNo ratings yet
- Surgical Notes (Teddy)Document88 pagesSurgical Notes (Teddy)shichianNo ratings yet
- SCHS Nursing Specialist Exam Revision 2Document18 pagesSCHS Nursing Specialist Exam Revision 2Ahmad Khalil Al Sadi70% (20)
- CSF Cell Count: How The Test Is PerformedDocument3 pagesCSF Cell Count: How The Test Is PerformedMars AqmalNo ratings yet
- Cholecystitis NCPDocument4 pagesCholecystitis NCPdark-canales33% (3)
- MR Loveday Little Outing Day AnalysisDocument4 pagesMR Loveday Little Outing Day AnalysisLorenaGeninSantaCruz40% (10)
- Pin Site CareDocument8 pagesPin Site Carernbell18013No ratings yet