You might also like
- AZ Lawbook PDFDocument240 pagesAZ Lawbook PDFEd ConwayNo ratings yet
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Infectious Diseases IDocument7 pagesInfectious Diseases ITiff VoNo ratings yet
- Aznan Lelo & Zulkarnain Rangkuty: Dep. Farmakologi & TerapeutikDocument52 pagesAznan Lelo & Zulkarnain Rangkuty: Dep. Farmakologi & TerapeutikPriawanIndraNo ratings yet
- Inhibitor of Cell Wall SynthesisDocument30 pagesInhibitor of Cell Wall SynthesisAditya BustamiNo ratings yet
- Mark Miguel P. Latras, RPHDocument11 pagesMark Miguel P. Latras, RPHLOLOLONo ratings yet
- Antibiotic FinalDocument58 pagesAntibiotic Finalvandana kethavathNo ratings yet
- Laboratory of Microbiology Medical Faculty UB 2009Document37 pagesLaboratory of Microbiology Medical Faculty UB 2009zianaNo ratings yet
- 2008 Block2 ReviewDocument28 pages2008 Block2 ReviewbellNo ratings yet
- AntimicrobialDocument211 pagesAntimicrobialSanaz Niksefat100% (1)
- Ab Betalactam 2Document30 pagesAb Betalactam 2NovianaHartikasariNo ratings yet
- Abfghx Cfghheat Shfgheet Abx QNDocument6 pagesAbfghx Cfghheat Shfgheet Abx QNRăzvan RoșcaNo ratings yet
- Anti Bio IticsDocument61 pagesAnti Bio IticsyangehmelvislimnyuyNo ratings yet
- Antibiotics: Faculty of Dentistry 22 September 2014Document61 pagesAntibiotics: Faculty of Dentistry 22 September 2014gamalsolimanNo ratings yet
- Antibiotics For PneumoniaDocument52 pagesAntibiotics For PneumoniaAndy DazNo ratings yet
- Antimicrobial Drugs: Laboratory of Microbiology Medical Faculty Brawijaya UniversityDocument38 pagesAntimicrobial Drugs: Laboratory of Microbiology Medical Faculty Brawijaya UniversityYuu Ayu'k LifestarNo ratings yet
- Prinsip Penggunaan Antibiotik Untuk Terapi: Khie ChenDocument66 pagesPrinsip Penggunaan Antibiotik Untuk Terapi: Khie ChenAnindia LarasatiNo ratings yet
- 05 抗生素簡介(上)Document64 pages05 抗生素簡介(上)ahmed.20hm13No ratings yet
- Chemotherapy: BY Professor Dr. Ahmed KhalilDocument29 pagesChemotherapy: BY Professor Dr. Ahmed KhalilSAYED ZAKINo ratings yet
- Ppra Ab Terapi PDFDocument83 pagesPpra Ab Terapi PDFDIONYSIUS BENINo ratings yet
- Ab Betalactam 2Document36 pagesAb Betalactam 2Anonymous QPakSNNo ratings yet
- Antibiotic in Daily Practice IARW 2017Document50 pagesAntibiotic in Daily Practice IARW 2017Benny Chris TantoNo ratings yet
- USMLE Step 3 Lecture Notes 2017-2018Document74 pagesUSMLE Step 3 Lecture Notes 2017-2018kaelenNo ratings yet
- Bagian Mikrobiologi Fk-Unhas 2007: Baedah MadjidDocument17 pagesBagian Mikrobiologi Fk-Unhas 2007: Baedah MadjidIsmail Sholeh Bahrun MakkaratteNo ratings yet
- Antimicrobialchemotheray PDFDocument80 pagesAntimicrobialchemotheray PDFغمدان دماج الحمزيNo ratings yet
- FINALS - Module 6Document29 pagesFINALS - Module 6Thereza CahigNo ratings yet
- 1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesDocument67 pages1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesadystiNo ratings yet
- In Et Ic S: To Xi Ci TyDocument63 pagesIn Et Ic S: To Xi Ci TyTsalitsa Nurramadhani MarjokoNo ratings yet
- Iii. Antibacterial DrugsDocument6 pagesIii. Antibacterial DrugskhaileenafaeNo ratings yet
- AntibioticsDocument101 pagesAntibioticsdentistmai24No ratings yet
- Anti Biotics & Lactam Antibiotics Visit For More Ppt'sDocument44 pagesAnti Biotics & Lactam Antibiotics Visit For More Ppt'sGANESH KUMAR JELLANo ratings yet
- AntibioticsDocument10 pagesAntibioticsStevhenson PortacioNo ratings yet
- 5) General BacteriologyDocument86 pages5) General BacteriologyIanBiagtanNo ratings yet
- Micro Bio paraDocument43 pagesMicro Bio paraMary Paula EstiveNo ratings yet
- Antimikroba-1Document21 pagesAntimikroba-1Richard MoralesNo ratings yet
- 2-Antibiotic ChemotherapyDocument34 pages2-Antibiotic ChemotherapyYoueel IbrahemNo ratings yet
- Betal Act A MineDocument44 pagesBetal Act A MineGeorgiana GoleaNo ratings yet
- CefalosporinasDocument12 pagesCefalosporinasVALENTINA ZAMBRANO ROMERONo ratings yet
- Penicillins Cephalosporins Monobactams CarbapenemsDocument77 pagesPenicillins Cephalosporins Monobactams CarbapenemsShehz BalochNo ratings yet
- Antimicrobial ChemotherapyDocument70 pagesAntimicrobial Chemotherapyamanialwerfalli4No ratings yet
- AntimikrobaDocument50 pagesAntimikrobaarisita firmanNo ratings yet
- Antibiotics F MCP 1Document37 pagesAntibiotics F MCP 1Mohamed ElraiyNo ratings yet
- Principles of Antibiotic TherapyDocument50 pagesPrinciples of Antibiotic TherapyMiaMDNo ratings yet
- Chemotherapy Lect 1Document26 pagesChemotherapy Lect 1kazelio2017No ratings yet
- 23 Antibiotics HandoutDocument14 pages23 Antibiotics HandoutMd Sakil AminNo ratings yet
- Antibiotics in Periodontal DiseaseDocument57 pagesAntibiotics in Periodontal DiseaseReshmaaRajendranNo ratings yet
- Penicillincephallosporine Beta Lactamase MonobactamDocument31 pagesPenicillincephallosporine Beta Lactamase Monobactamh210053mNo ratings yet
- ChemotherapyDocument253 pagesChemotherapyalmskein100% (1)
- 19 - ChemotherapyDocument38 pages19 - ChemotherapymeshoshalabyNo ratings yet
- Penicillins and Other Beta Lactam AntibioticsDocument67 pagesPenicillins and Other Beta Lactam AntibioticsAdina IqbalNo ratings yet
- Assessment Micro 2016 Clin CorDocument28 pagesAssessment Micro 2016 Clin CorPerlie CNo ratings yet
- Antibiotics 2Document31 pagesAntibiotics 2zainab ElsayedNo ratings yet
- Antimicrobial Chemotherapy IDocument30 pagesAntimicrobial Chemotherapy Inighat khanNo ratings yet
- AntibioticsDocument9 pagesAntibioticsprince1500100% (1)
- 2 Beta Lactum 2020Document25 pages2 Beta Lactum 2020Sparks Francis EzikaNo ratings yet
- Inhibitor of Cell Wall SynthesisDocument30 pagesInhibitor of Cell Wall SynthesisjyuldipNo ratings yet
- 2.2.4 - Cell Wall Inhibitors - Cephalosporines 2010-Oct 2014Document25 pages2.2.4 - Cell Wall Inhibitors - Cephalosporines 2010-Oct 2014tresorstephane669No ratings yet
- Inhibit Classification AntibioticsDocument5 pagesInhibit Classification AntibioticsNurnaningsi Tajuddin ThalibNo ratings yet
- Infectious Hour (Antibiotics)Document90 pagesInfectious Hour (Antibiotics)Jill PardoNo ratings yet
- Penicillin G Ampicillin: AmoxilDocument17 pagesPenicillin G Ampicillin: AmoxilSolomon Seth SallforsNo ratings yet
- Classification of Clinically Significant Bacteria by GenusDocument2 pagesClassification of Clinically Significant Bacteria by GenusSEAN BUINo ratings yet
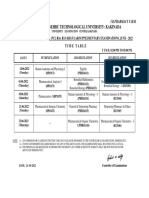
- JNTUK B.pharmacy 1-1 TT June 2022Document1 pageJNTUK B.pharmacy 1-1 TT June 2022princepharmaa13No ratings yet
- Pharmacology AbbreviationsDocument2 pagesPharmacology AbbreviationsChiisanaPlays LIFEAFTERNo ratings yet
- Split Decisions:: FDA Provides More Direction As Questions Arise About Dosage ConsistencyDocument2 pagesSplit Decisions:: FDA Provides More Direction As Questions Arise About Dosage ConsistencyCYBERPHARMNo ratings yet
- H01043-Hoá Dư C 2-Lecture 6-AntidepressantsDocument26 pagesH01043-Hoá Dư C 2-Lecture 6-AntidepressantsKTrọng NghĩaNo ratings yet
- Drugs Acting On Immune SystemDocument6 pagesDrugs Acting On Immune SystemSORENI SORENINo ratings yet
- Daftar Pustaka: RETIKA GIEN SYAPUTRI, Angi Nadya Bestari, M.SC., AptDocument8 pagesDaftar Pustaka: RETIKA GIEN SYAPUTRI, Angi Nadya Bestari, M.SC., Aptsiska putri utamaNo ratings yet
- Farmaceuti I Njihova Karijera KEY WORDSDocument3 pagesFarmaceuti I Njihova Karijera KEY WORDSŽivana PopićNo ratings yet
- Register, 2012Document233 pagesRegister, 2012Natalia Pika Ambrace0% (1)
- Market Reflection Report Mar'20Document24 pagesMarket Reflection Report Mar'20Stevin George100% (1)
- Veterinary Medicines: A Compact Collection of Information On Veterinary Drugs/medicines in PracticeDocument64 pagesVeterinary Medicines: A Compact Collection of Information On Veterinary Drugs/medicines in Practiceomprakash Chabarwal100% (1)
- 0900 1030 Nicolette Graham PDFDocument28 pages0900 1030 Nicolette Graham PDFhinaNo ratings yet
- Intern Chap 3-4Document2 pagesIntern Chap 3-4Marc HenryNo ratings yet
- Dangerous Drug Act (DDA) Cap 134Document4 pagesDangerous Drug Act (DDA) Cap 134hiiiiNo ratings yet
- Report of Analysis: EL/I/15/ 06.2820 Air Limbah Waste WaterDocument2 pagesReport of Analysis: EL/I/15/ 06.2820 Air Limbah Waste WatergintaniNo ratings yet
- Anxiolytic and Hypnotic DrugsDocument6 pagesAnxiolytic and Hypnotic DrugsFalah Dakka100% (2)
- KACH Formulary Category OCT09Document5 pagesKACH Formulary Category OCT09dareesNo ratings yet
- Muslim Contributions To ScienceDocument164 pagesMuslim Contributions To ScienceNixbie (Pemula yg serba Kepo)No ratings yet
- SPH Untuk Rsud BKKMDocument57 pagesSPH Untuk Rsud BKKMBagas PutranandaNo ratings yet
- Prescription For Addiction: UpdateDocument8 pagesPrescription For Addiction: Updateoptions1No ratings yet
- CNS Drugs Pharmaceutical Form Therapeutic Group: 6mg, 8mgDocument7 pagesCNS Drugs Pharmaceutical Form Therapeutic Group: 6mg, 8mgCha GabrielNo ratings yet
- Quality Circle For GenericsDocument38 pagesQuality Circle For GenericsAngelica BolosNo ratings yet
- SIFM PharmRevisedAPPENDIX-BDocument16 pagesSIFM PharmRevisedAPPENDIX-Bmonish reddyNo ratings yet
- Kelompok 4 - Accepting A New PatientDocument16 pagesKelompok 4 - Accepting A New PatientSiti rohaniNo ratings yet
- Jenis Persediaan Barang Habis Pakai Satuan Harga Nama BHN Baku Obat Total Kebutuhan 1 TH FarmasiDocument22 pagesJenis Persediaan Barang Habis Pakai Satuan Harga Nama BHN Baku Obat Total Kebutuhan 1 TH FarmasiLusi LestariNo ratings yet
- FDA Orphan Drug ReviewDocument49 pagesFDA Orphan Drug ReviewpdgcssNo ratings yet
- Pharmaceutical Science 2014Document24 pagesPharmaceutical Science 2014lovehope100% (1)
- Pharmacology MCQS1Document11 pagesPharmacology MCQS1Y Sp2No ratings yet
- Atrial Fibrilasi RATE CONTROL (Target HR 110 BPM)Document5 pagesAtrial Fibrilasi RATE CONTROL (Target HR 110 BPM)Melani NauritaNo ratings yet
- JMP - Life Sciences - Schedule - 06-14-19Document2 pagesJMP - Life Sciences - Schedule - 06-14-19akNo ratings yet