You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Voter ListDocument214 pagesVoter ListMadhu Sudhan PandeyaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Abortion: Renhe Hospital Wang JunjieDocument51 pagesAbortion: Renhe Hospital Wang JunjieMadhu Sudhan PandeyaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Quick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountDocument2 pagesQuick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountMadhu Sudhan Pandeya100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Lecture-31 Instrumental DeliveryDocument33 pagesLecture-31 Instrumental DeliveryMadhu Sudhan PandeyaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Nepal Medical Council Act, 2020 (1964)Document20 pagesNepal Medical Council Act, 2020 (1964)Madhu Sudhan PandeyaNo ratings yet
- Lecture-28 Placenta PreviaDocument43 pagesLecture-28 Placenta PreviaMadhu Sudhan Pandeya100% (1)
- Teratology & Chronic PoisoningDocument54 pagesTeratology & Chronic PoisoningMadhu Sudhan PandeyaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Postpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinDocument98 pagesPostpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinMadhu Sudhan PandeyaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Lecture-35 Eectronic Fetal MonitoringDocument45 pagesLecture-35 Eectronic Fetal MonitoringMadhu Sudhan PandeyaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Lecture-11 Breech PresentationDocument27 pagesLecture-11 Breech PresentationMadhu Sudhan PandeyaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Vaccination Guideline: International Travel and Health 2007Document9 pagesVaccination Guideline: International Travel and Health 2007Madhu Sudhan PandeyaNo ratings yet
- Lecture-33 Postpartum HemorrhageDocument50 pagesLecture-33 Postpartum HemorrhageMadhu Sudhan Pandeya100% (2)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Lecture-4 Diagnosis of PregnancyDocument31 pagesLecture-4 Diagnosis of PregnancyMadhu Sudhan Pandeya100% (1)
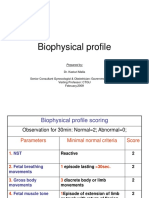
- Lecture-23 Biophysical ProfieDocument3 pagesLecture-23 Biophysical ProfieMadhu Sudhan PandeyaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Lecture-25 Cesarean SectionDocument21 pagesLecture-25 Cesarean SectionMadhu Sudhan PandeyaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Lecture-17 Shoulder DystociaDocument20 pagesLecture-17 Shoulder DystociaMadhu Sudhan PandeyaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Lecture-22 Prolonged PregnancyDocument24 pagesLecture-22 Prolonged PregnancyMadhu Sudhan PandeyaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Lecture-26 Hypertensive Disease of PregnancyDocument28 pagesLecture-26 Hypertensive Disease of PregnancyMadhu Sudhan PandeyaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Bishop's Pre-Induction Cervical Scoring SystemDocument2 pagesBishop's Pre-Induction Cervical Scoring SystemMadhu Sudhan PandeyaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lecture-13 Transeverse LieDocument15 pagesLecture-13 Transeverse LieMadhu Sudhan PandeyaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Lecture-18 Obstructed LaborDocument8 pagesLecture-18 Obstructed LaborMadhu Sudhan PandeyaNo ratings yet
- Lecture-12 Face PresentationDocument9 pagesLecture-12 Face PresentationMadhu Sudhan PandeyaNo ratings yet
- Lecture-15 Prolonged LaborDocument8 pagesLecture-15 Prolonged LaborMadhu Sudhan PandeyaNo ratings yet
- Antenatal Care and High Risk PregnancyDocument12 pagesAntenatal Care and High Risk PregnancyMadhu Sudhan PandeyaNo ratings yet
- Lecture-24 Twins PregnancyDocument30 pagesLecture-24 Twins PregnancyMadhu Sudhan PandeyaNo ratings yet
- Lecture-8 First Stage ManagementDocument10 pagesLecture-8 First Stage ManagementMadhu Sudhan PandeyaNo ratings yet
- Lecture-20 Premature LaborDocument13 pagesLecture-20 Premature LaborMadhu Sudhan PandeyaNo ratings yet
- Organophosphate PoisoningDocument40 pagesOrganophosphate PoisoningMadhu Sudhan PandeyaNo ratings yet
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Lecture-10 EpisiotomyDocument11 pagesLecture-10 EpisiotomyMadhu Sudhan Pandeya67% (3)
- 9201 Mark Scheme Paper2 International Gcse Biology Jun22Document21 pages9201 Mark Scheme Paper2 International Gcse Biology Jun22asdf0% (1)
- NBECT Handout 12 INDUSTRIAL BIOTECHNOLOGYDocument16 pagesNBECT Handout 12 INDUSTRIAL BIOTECHNOLOGYAlliana EclarinalNo ratings yet
- Exam I Questions 01Document31 pagesExam I Questions 01bravdaNo ratings yet
- Englidh Sample Question PaperDocument13 pagesEnglidh Sample Question PaperUtkarsh TewariNo ratings yet
- Homework 18.1: Biodiversity, Classification and ConservationDocument2 pagesHomework 18.1: Biodiversity, Classification and ConservationMikeNo ratings yet
- Pena V Youngkin - Amended Writ For Pena V NorthamDocument62 pagesPena V Youngkin - Amended Writ For Pena V NorthamAnthony DocKek PenaNo ratings yet
- HES 032 - SAS 1 - Merged-3Document1 pageHES 032 - SAS 1 - Merged-3bangtanswifue -No ratings yet
- Machupo VirusDocument15 pagesMachupo VirusiggyNo ratings yet
- Rabies: Dr. Paul Bartlett, MPH., DVM., PH.DDocument45 pagesRabies: Dr. Paul Bartlett, MPH., DVM., PH.DnfrnufaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CHN Lecture Note For Set 24 Student NursesDocument37 pagesCHN Lecture Note For Set 24 Student NursesYahya Ahmad SulaimamNo ratings yet
- Klasifikasi VirusDocument3 pagesKlasifikasi VirusADINo ratings yet
- Directed Reading CH 15Document2 pagesDirected Reading CH 15Ismail Medhat SalahNo ratings yet
- Dengue Fever PDFDocument8 pagesDengue Fever PDFushapadminivadivelswamyNo ratings yet
- Environmental Microbiology: Third EditionDocument18 pagesEnvironmental Microbiology: Third EditionCarlos Israel Esparza Andrade50% (2)
- For The Orthodox Faithful Who Are Confused About COVID VaccinesDocument11 pagesFor The Orthodox Faithful Who Are Confused About COVID VaccinesAleksander RizjaNo ratings yet
- LABORATORY MANUAL Plant and Animal SystematicsDocument10 pagesLABORATORY MANUAL Plant and Animal SystematicsAnisJasminAziminNo ratings yet
- Viral Genetics and Replication 2Document13 pagesViral Genetics and Replication 2ميمونه عبد الرحيم مصطفىNo ratings yet
- What Is Immunotherapy?Document19 pagesWhat Is Immunotherapy?Najia ChoudhuryNo ratings yet
- Interpreting Covid-19 Test Results: Guidance OnDocument1 pageInterpreting Covid-19 Test Results: Guidance OnromalejNo ratings yet
- Obama SUED Using Bio-Terrorism For Mass Genocide Against The U.S. PopulationDocument6 pagesObama SUED Using Bio-Terrorism For Mass Genocide Against The U.S. PopulationLevitator100% (7)
- Beasts of The Earth Animals, Humans, and DiseaseDocument206 pagesBeasts of The Earth Animals, Humans, and Diseasehadrian75100% (1)
- Biology Midterm 2023Document18 pagesBiology Midterm 2023Hellen LiuNo ratings yet
- VIRUSESDocument29 pagesVIRUSEStria nurdianaNo ratings yet
- Infection Basics: Biology 4310 Virology Spring 2020Document49 pagesInfection Basics: Biology 4310 Virology Spring 2020Robin SinghNo ratings yet
- Austin Journal of Plant BiologyDocument4 pagesAustin Journal of Plant BiologyAustin Publishing GroupNo ratings yet
- Plant Disease Detection Using Image ProcessingDocument5 pagesPlant Disease Detection Using Image ProcessingTest Email100% (1)
- Prescott's Microbiology, 12th Edition TEST BANK by Joanne Willey Verified Chapter's 1 - 42 CompleteDocument70 pagesPrescott's Microbiology, 12th Edition TEST BANK by Joanne Willey Verified Chapter's 1 - 42 Completemarcuskenyatta275No ratings yet
- MCQ InfectionsDocument10 pagesMCQ Infectionsعلي الكوافيNo ratings yet
- Cationic Lipospheres As Delivery Systems For Nucleic Acid MoleculesDocument17 pagesCationic Lipospheres As Delivery Systems For Nucleic Acid Moleculesdepardieu1973No ratings yet
- Small Pox Is DeadDocument46 pagesSmall Pox Is Deadtummalapalli venkateswara raoNo ratings yet