You might also like
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- Patient safety protocols in the operating theatreDocument36 pagesPatient safety protocols in the operating theatreDewa DyskaNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- Nursing Staff & Anesthesia Technicians in DPUDocument10 pagesNursing Staff & Anesthesia Technicians in DPUnasserjubranNo ratings yet
- Robotic Hernia Surgery: A Comprehensive Illustrated GuideFrom EverandRobotic Hernia Surgery: A Comprehensive Illustrated GuideOmar Yusef KudsiNo ratings yet
- Operating Room ExperienceDocument7 pagesOperating Room ExperienceDequnda SmithNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Aakash Patient Care Services AssingmentDocument10 pagesAakash Patient Care Services Assingmentaakash sharmaNo ratings yet
- JCI PresentationDocument66 pagesJCI PresentationOsama MarzoukNo ratings yet
- IPSG 2020 Accreditation OverviewDocument17 pagesIPSG 2020 Accreditation OverviewNicole KrishnaNo ratings yet
- Pre Op MNGMNTDocument22 pagesPre Op MNGMNTsandeepv08No ratings yet
- Surgical Site Marking Procedure GuideDocument4 pagesSurgical Site Marking Procedure GuideSony PrabowoNo ratings yet
- Case Study 2014Document56 pagesCase Study 2014amier_s100% (1)
- Essential Intraoperative Nursing Care for Hernia Repair PatientDocument4 pagesEssential Intraoperative Nursing Care for Hernia Repair PatientGia Lourdes Camille AustriaNo ratings yet
- Ministry of Health and Family Welfare: Safe Surgery Checklist: User GuideDocument2 pagesMinistry of Health and Family Welfare: Safe Surgery Checklist: User GuideShahidul Islam ChowdhuryNo ratings yet
- NURSING-Operating Room ObservationDocument7 pagesNURSING-Operating Room ObservationNeema NimuNo ratings yet
- Ipsg 2017Document41 pagesIpsg 2017hum JavedNo ratings yet
- Patient SafetyDocument22 pagesPatient SafetyRensy Sabi100% (1)
- Surgical SafetyDocument23 pagesSurgical SafetyNimi BatuboNo ratings yet
- 16/12/12 Army Force Comphensive Specialized Hospital or Department Standard /sop/ Nursing DutiesDocument7 pages16/12/12 Army Force Comphensive Specialized Hospital or Department Standard /sop/ Nursing DutiesSuzy BaeNo ratings yet
- Periop 8Document18 pagesPeriop 8Bern GervacioNo ratings yet
- New Operating Room Protocol That May Save Your LifeDocument15 pagesNew Operating Room Protocol That May Save Your Lifebibot1No ratings yet
- OR Duty RLE RequirementsDocument5 pagesOR Duty RLE RequirementsSammy Jr FamilarNo ratings yet
- Module 2Document2 pagesModule 2Duchess Juliane Jose MirambelNo ratings yet
- Procedural Verification ProtocolDocument4 pagesProcedural Verification ProtocolPops IcunaNo ratings yet
- Scheduling of Patients For SurgeryDocument7 pagesScheduling of Patients For SurgeryAllein Antonio-GeganteNo ratings yet
- Task 10Document8 pagesTask 10rashiNo ratings yet
- Session 2Document5 pagesSession 2Sistine Rose LabajoNo ratings yet
- Documented Procedure Addresses The Prevention of Adverse Events Like Wrong Site, Wrong Patient and Wrong SurgeryDocument10 pagesDocumented Procedure Addresses The Prevention of Adverse Events Like Wrong Site, Wrong Patient and Wrong SurgeryPamukuntla MounikareddyNo ratings yet
- Wound ManaagementDocument20 pagesWound Manaagementandrewonguka9No ratings yet
- Powerpoint Correct OperationDocument41 pagesPowerpoint Correct OperationMary MathewsNo ratings yet
- Red Blanket Protocol RBWHDocument3 pagesRed Blanket Protocol RBWHLanga LutshabaNo ratings yet
- "Time-Out" in Surgical Operation: Student's Name: Institution: Course: DateDocument4 pages"Time-Out" in Surgical Operation: Student's Name: Institution: Course: DateMzunguNo ratings yet
- Day 1 ConceptDocument45 pagesDay 1 ConceptRamzen Raphael DomingoNo ratings yet
- Sas 2 Cabahug, Victoria Mae IDocument4 pagesSas 2 Cabahug, Victoria Mae Ibekbekk cabahugNo ratings yet
- Medical Surgical Nursing ConceptsDocument45 pagesMedical Surgical Nursing ConceptsKristel Anne100% (1)
- Patient Care Delivery and Safety StandardsDocument4 pagesPatient Care Delivery and Safety StandardsANDREW DEL ROSARIONo ratings yet
- Surgery RobaDocument26 pagesSurgery Robaroba shukreNo ratings yet
- Peran - Fungsi Perawat Safe SurgeryDocument69 pagesPeran - Fungsi Perawat Safe Surgeryerwin salehNo ratings yet
- TIME OUT OpoDocument7 pagesTIME OUT OpoDiego BrecedaNo ratings yet
- Module 1 Case StudyDocument7 pagesModule 1 Case StudyDivine ParagasNo ratings yet
- Word Perioperative NursingDocument19 pagesWord Perioperative NursingGerald Resubal Oriña100% (1)
- Management of OP Waiting Areas SOP 201120 - CurrentDocument4 pagesManagement of OP Waiting Areas SOP 201120 - CurrentJehad Al yousefNo ratings yet
- Pre and Post Op Care: by Elaine Jones + Anne WrightDocument29 pagesPre and Post Op Care: by Elaine Jones + Anne WrightSarah Eddiah100% (3)
- Lecture 23Document28 pagesLecture 23Danica PelegrinoNo ratings yet
- Surgical Safety ChecklistDocument16 pagesSurgical Safety ChecklistHafizur Rashid100% (1)
- Univ ProtocolDocument4 pagesUniv ProtocolandryshevNo ratings yet
- Nursing Midwifery Staff CBAHI QuestionsDocument13 pagesNursing Midwifery Staff CBAHI QuestionsnasserjubranNo ratings yet
- Alexanders Care Patient Surgery 16th Rothrock Test BankDocument10 pagesAlexanders Care Patient Surgery 16th Rothrock Test BankfahedqNo ratings yet
- Sample Ophthalmology ChecklistDocument3 pagesSample Ophthalmology ChecklistParas AgarwalNo ratings yet
- OR RotationDocument20 pagesOR RotationJestine Joy CustodioNo ratings yet
- Perioperative: Operating Room AttireDocument95 pagesPerioperative: Operating Room AttireCristina Tagle GarciaNo ratings yet
- 10 1005 - Continuous Patient MonitoringDocument3 pages10 1005 - Continuous Patient MonitoringChristian KleinNo ratings yet
- The Perioperative Nurse's Duties and Responsibilities: Surgical Nursing DefinedDocument9 pagesThe Perioperative Nurse's Duties and Responsibilities: Surgical Nursing DefinedSiena Lou CeniaNo ratings yet
- Theatre Nursing 4 1Document98 pagesTheatre Nursing 4 1Priscah bhokeNo ratings yet
- Best Practices To Prevent RSIDocument53 pagesBest Practices To Prevent RSIDevi Putri100% (1)
- Hospital SopsDocument12 pagesHospital Sopspratimaz80% (5)
- Role of Perioperative NurseDocument30 pagesRole of Perioperative Nursealiyemany23No ratings yet
- Infofrafia NchaDocument11 pagesInfofrafia NchaDARWUING JOSE ACUÑA CABANILLASNo ratings yet
- Cochlear Implant GuidelinesDocument29 pagesCochlear Implant GuidelinesArun PatoleNo ratings yet
- CMS CastleDocument5 pagesCMS CastleKian GonzagaNo ratings yet
- 000 Holy Saturday Extract From Priest Altar BookDocument45 pages000 Holy Saturday Extract From Priest Altar BookKian GonzagaNo ratings yet
- Psalm and POFDocument1 pagePsalm and POFKian GonzagaNo ratings yet
- CMS CastleDocument5 pagesCMS CastleKian GonzagaNo ratings yet
- Basic Airway ManagmentDocument28 pagesBasic Airway ManagmentKian GonzagaNo ratings yet
- 002 Exsultet Choir PartsDocument2 pages002 Exsultet Choir PartsKian GonzagaNo ratings yet
- 001 The Light of ChristDocument1 page001 The Light of ChristKian GonzagaNo ratings yet
- Revised Bishop Installation MassDocument43 pagesRevised Bishop Installation MassKian GonzagaNo ratings yet
- LS Intuity The Server Getting-StartedDocument38 pagesLS Intuity The Server Getting-StartedKian GonzagaNo ratings yet
- O Come, Let Us Adore Him (x3) Christ The LordDocument3 pagesO Come, Let Us Adore Him (x3) Christ The LordKian GonzagaNo ratings yet
- Highlights+Bar+Menu+ +With+Price+March+2021Document2 pagesHighlights+Bar+Menu+ +With+Price+March+2021Kian GonzagaNo ratings yet
- Christmas Carol Songbook SATB PDFDocument24 pagesChristmas Carol Songbook SATB PDFPrecious Caperocho100% (1)
- Firmly I Believe - SEMS - SATBDocument1 pageFirmly I Believe - SEMS - SATBKian GonzagaNo ratings yet
- We Adore YouDocument1 pageWe Adore YouKian GonzagaNo ratings yet
- Learningspace Troubleshooting Guide: - Start HereDocument1 pageLearningspace Troubleshooting Guide: - Start HereKian GonzagaNo ratings yet
- Orient+Lounge+Bar+Menu+ +With+Price+March+2021Document1 pageOrient+Lounge+Bar+Menu+ +With+Price+March+2021Kian GonzagaNo ratings yet
- Easter Sun 6A - Ps 65 (66) - Part 1Document1 pageEaster Sun 6A - Ps 65 (66) - Part 1Kian GonzagaNo ratings yet
- Check Out Our Digital Menus: Just Scan or Click On Below QR CodesDocument1 pageCheck Out Our Digital Menus: Just Scan or Click On Below QR CodesKian GonzagaNo ratings yet
- Guidelines Liturgical MusicDocument160 pagesGuidelines Liturgical MusicJerahmel Vincent Abueva Cofreros100% (1)
- RPSI+ +Welcome+Letter+ +2021Document2 pagesRPSI+ +Welcome+Letter+ +2021Kian GonzagaNo ratings yet
- Course: Patient Safety Solutions Topic:: Some DefinitionsDocument5 pagesCourse: Patient Safety Solutions Topic:: Some DefinitionsKian GonzagaNo ratings yet
- User Manual: Register Pay LearnDocument21 pagesUser Manual: Register Pay LearnKian GonzagaNo ratings yet
- Light Vehicle Driving Course Safety SkillsDocument8 pagesLight Vehicle Driving Course Safety SkillsKian GonzagaNo ratings yet
- ChargeTech PLUG Manual - 42K & 54KDocument6 pagesChargeTech PLUG Manual - 42K & 54KKian GonzagaNo ratings yet
- Misa Immaculada Concepcion PDFDocument90 pagesMisa Immaculada Concepcion PDFArlie Torres100% (1)
- Abu Dhabi Stem Cells Center Lab ReportDocument1 pageAbu Dhabi Stem Cells Center Lab ReportKian GonzagaNo ratings yet
- 2021 USCCB Liturgical CalendarDocument52 pages2021 USCCB Liturgical Calendartmptpaul100% (1)
- Specs Features: FrameDocument1 pageSpecs Features: FrameKian GonzagaNo ratings yet
- User Guide On How To Generate PDF Versions of The Product Information and Other Annexes PDFDocument11 pagesUser Guide On How To Generate PDF Versions of The Product Information and Other Annexes PDFba7r7737No ratings yet
- Bike Shop - MAP - 2020Document1 pageBike Shop - MAP - 2020Kian GonzagaNo ratings yet
- Project ProposalDocument16 pagesProject ProposalMashaal FasihNo ratings yet
- Grief & Grieving ProcessDocument39 pagesGrief & Grieving Processelmerconde100% (4)
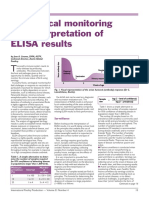
- Serological Monitoring by ELISADocument3 pagesSerological Monitoring by ELISAreza tavayef100% (1)
- NCM 101 Vital Signs PPT BSN 1a Group 1Document138 pagesNCM 101 Vital Signs PPT BSN 1a Group 1Brian Anthony100% (1)
- West Fertilizer FINAL Report For Website 0223161 PDFDocument267 pagesWest Fertilizer FINAL Report For Website 0223161 PDFJawahar KhetanNo ratings yet
- Cysts of The JawsDocument75 pagesCysts of The JawsSwetha KaripineniNo ratings yet
- Designsolutions 2010springDocument68 pagesDesignsolutions 2010springjkarpitskiyNo ratings yet
- Vitamin Water - Arnel Ricafranca PDFDocument32 pagesVitamin Water - Arnel Ricafranca PDFAlaa EssamNo ratings yet
- The Northern Ireland Sport and Physical Activity Survey 2010 (SAPAS)Document178 pagesThe Northern Ireland Sport and Physical Activity Survey 2010 (SAPAS)sportniNo ratings yet
- Eshre Guideline Endometriosis 2022Document192 pagesEshre Guideline Endometriosis 2022Patricia100% (1)
- Cuplocks Scaffolding JSA UtilityDocument4 pagesCuplocks Scaffolding JSA UtilitysoubhagyaNo ratings yet
- The30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Document17 pagesThe30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Alexander OrzocoNo ratings yet
- Berklee Intro Music Therapy PDFDocument17 pagesBerklee Intro Music Therapy PDFTheodore VaillantNo ratings yet
- 100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFDocument12 pages100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFJawad AkbarNo ratings yet
- Municipality of Naic, Cavite Gender and Development Plan: Programs / Projects / Activities Appropriation ObligationDocument2 pagesMunicipality of Naic, Cavite Gender and Development Plan: Programs / Projects / Activities Appropriation Obligationbunso2012No ratings yet
- MSDS for Feldspar PowderDocument7 pagesMSDS for Feldspar PowderRıdvan SürmeliNo ratings yet
- Unit 4 CommunicationDocument3 pagesUnit 4 Communicationsutarmisaja15No ratings yet
- Managing STEM AthletesDocument13 pagesManaging STEM Athletesanon_629662799No ratings yet
- Human Performance - MITRE CorporationDocument90 pagesHuman Performance - MITRE CorporationCantankerous BuddhaNo ratings yet
- AOTA Statement On Role of OT in NICUDocument9 pagesAOTA Statement On Role of OT in NICUMapi RuizNo ratings yet
- Trays PDFDocument18 pagesTrays PDFBilal Hasan100% (1)
- Theory Critique of Boundaries in MarriageDocument8 pagesTheory Critique of Boundaries in MarriagepatrickakingNo ratings yet
- Introduction of Online Basic First Aid Course - For Circulation April 2021Document39 pagesIntroduction of Online Basic First Aid Course - For Circulation April 2021Yuwaraj NaiduNo ratings yet
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
- (Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioDocument455 pages(Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioEsteban Gonzàlez RodriguezNo ratings yet
- Case Study (Amit Mandal)Document7 pagesCase Study (Amit Mandal)Mukesh SelvanNo ratings yet
- Health and Safety Standards in D&TDocument9 pagesHealth and Safety Standards in D&TAnnie HawkinsNo ratings yet
- MSDSDocument3 pagesMSDSSiti Nurjanah SeptianiNo ratings yet
- Grizz Phys Tier 2 PDFDocument19 pagesGrizz Phys Tier 2 PDFJ VivianNo ratings yet
- Unit 1-Omd553-Telehealth TechnologyDocument53 pagesUnit 1-Omd553-Telehealth TechnologyjgjeslinNo ratings yet