You might also like
- Crohns Disease FinalDocument3 pagesCrohns Disease Finalapi-535481376No ratings yet
- Chapter 12 GastrointestinalDocument11 pagesChapter 12 GastrointestinalRaju NiraulaNo ratings yet
- Drug Study AssignmentDocument1 pageDrug Study AssignmentDaniela Claire FranciscoNo ratings yet
- Drug Study AssignmentDocument1 pageDrug Study AssignmentDaniela Claire FranciscoNo ratings yet
- Drug Study: 10cc/1vialDocument2 pagesDrug Study: 10cc/1vialJoevence Gazo CuaresmaNo ratings yet
- Omeprazol - Drug StudyDocument2 pagesOmeprazol - Drug StudyMae Visperas100% (1)
- 3.3 Medication Histories of Peptic Ulcer Disease: Table 3.3aDocument10 pages3.3 Medication Histories of Peptic Ulcer Disease: Table 3.3ab_rahman2k39603No ratings yet
- Mindanao State University - Iligan Institute of Technology: Drug StudyDocument3 pagesMindanao State University - Iligan Institute of Technology: Drug StudyAkiraMamoNo ratings yet
- Name of DrugDocument6 pagesName of DrugKathleen ColinioNo ratings yet
- Generic Name: General Indications More CommonDocument10 pagesGeneric Name: General Indications More CommonRosenda GonzalesNo ratings yet
- Drug Study Kathleen Claire ColinioDocument11 pagesDrug Study Kathleen Claire ColinioKathleen ColinioNo ratings yet
- Famotidine CompressDocument1 pageFamotidine CompressAlyssa Marie PepitoNo ratings yet
- MetoclopramideDocument1 pageMetoclopramideJack SolomonNo ratings yet
- Tangina Mo BizarDocument1 pageTangina Mo BizarJhon eric EscultorNo ratings yet
- Famotidine CompressDocument1 pageFamotidine CompressAlyssa Marie PepitoNo ratings yet
- Carbamazepine Drug StudyDocument2 pagesCarbamazepine Drug StudyMariel Raven ValdezNo ratings yet
- Antidepressant Comparison ChartDocument3 pagesAntidepressant Comparison Chartiggyputtty100% (29)
- Antibiotic Moa Mor Indication Formulation/ Dose Typical Sensitivities Adverse Effects Interactions Other InfoDocument2 pagesAntibiotic Moa Mor Indication Formulation/ Dose Typical Sensitivities Adverse Effects Interactions Other Infokalli987No ratings yet
- Heparin and WarfarinDocument3 pagesHeparin and WarfarinannieNo ratings yet
- Drugs Pharmacokinetics Indications Contraindicatio N Interaction Adverse Effects Generic NameDocument1 pageDrugs Pharmacokinetics Indications Contraindicatio N Interaction Adverse Effects Generic NameJR BetonioNo ratings yet
- M.I. (Losartan) Drug Study)Document2 pagesM.I. (Losartan) Drug Study)Angelica Marie MacaslingNo ratings yet
- Dopamine Antagonist: Generic Name: Chemical EffectDocument2 pagesDopamine Antagonist: Generic Name: Chemical EffectMajeed AlzahraniNo ratings yet
- Drugs For Treatment of PCPDocument5 pagesDrugs For Treatment of PCPwennyoktavNo ratings yet
- TB DRUGS 2023-2024 SummaryDocument4 pagesTB DRUGS 2023-2024 SummaryMark Lorenz NaldozaNo ratings yet
- Omeprazole Drug StudyDocument4 pagesOmeprazole Drug StudyjoanneNo ratings yet
- Drug Classification Mechanism of Action Indication Contraindication Adverse Effects Nursing ResponsibilitiesDocument17 pagesDrug Classification Mechanism of Action Indication Contraindication Adverse Effects Nursing ResponsibilitiesAsterlyn ConiendoNo ratings yet
- Pharmacology Concise Notes NEET-PGDocument30 pagesPharmacology Concise Notes NEET-PGMohamed TayyabNo ratings yet
- Observe Patient's 10 Rights of Medication AdministrationDocument2 pagesObserve Patient's 10 Rights of Medication AdministrationRyan Paul BalotNo ratings yet
- Lactulose: (Enuluse, Kristalose, Duphalac, Chronulac Syrup)Document30 pagesLactulose: (Enuluse, Kristalose, Duphalac, Chronulac Syrup)FEllis LEoNo ratings yet
- Nutriton - Charts Test 2Document3 pagesNutriton - Charts Test 2api-26938624No ratings yet
- Antihistamine Dose ChartDocument1 pageAntihistamine Dose ChartKerin KNo ratings yet
- Drug Study - OmeprazoleDocument5 pagesDrug Study - OmeprazoleRonel ResurricionNo ratings yet
- ONA Foundation DAILY Outpatient CENSUS (November 2018) Chief Complaint Diagnosis Management DAY 6 - November 21, 2018Document4 pagesONA Foundation DAILY Outpatient CENSUS (November 2018) Chief Complaint Diagnosis Management DAY 6 - November 21, 2018Ray Christoffer GomezNo ratings yet
- ICE DrugsDocument2 pagesICE DrugsRichelle FrondaNo ratings yet
- Drug StudyDocument8 pagesDrug StudyCourtney Dela FierraNo ratings yet
- Table 26-1. Classification and Comparison of Nonsteroidal AnalgesicsDocument11 pagesTable 26-1. Classification and Comparison of Nonsteroidal AnalgesicsAldy BimaNo ratings yet
- ND RDDocument10 pagesND RDOdyNo ratings yet
- Oncology Cheat Sheets - 1Document5 pagesOncology Cheat Sheets - 1abdallahmaurice94No ratings yet
- Bicalutamide (Casodex) Drug StudyDocument2 pagesBicalutamide (Casodex) Drug StudyAtteya Mogote AbdullahNo ratings yet
- Symptom Management Obstruksi BowelDocument5 pagesSymptom Management Obstruksi BowelPutri Mega PetasiNo ratings yet
- MirtazapineDocument4 pagesMirtazapineElyhna Mara U. Gonzales100% (1)
- Analgesia For InternsDocument4 pagesAnalgesia For InternsjsdlzjNo ratings yet
- DS 3 Ectopic PregnancyDocument2 pagesDS 3 Ectopic PregnancyJohn Kenley FerryNo ratings yet
- Drug Study (Covid Case)Document5 pagesDrug Study (Covid Case)YessaminNo ratings yet
- Bro Van ADocument2 pagesBro Van Asultan_bagadNo ratings yet
- Ultimate Pharmacoogy Guide PDFDocument18 pagesUltimate Pharmacoogy Guide PDFElizabella Henrietta TanaquilNo ratings yet
- HelminthsDocument11 pagesHelminthsTienneNo ratings yet
- Laboratory, Diagnostics Procedures & ConsultationDocument5 pagesLaboratory, Diagnostics Procedures & Consultationeva cortezNo ratings yet
- HIV Drug Chart (2021)Document1 pageHIV Drug Chart (2021)savNo ratings yet
- Medication Administration WorksheetDocument6 pagesMedication Administration WorksheetCheska CarrionNo ratings yet
- CheatDocument6 pagesCheatJona Rhose GadotNo ratings yet
- Drug StudyDocument7 pagesDrug StudyShem DelolaNo ratings yet
- Critical Care Drug Reference SheetDocument12 pagesCritical Care Drug Reference SheetYanina CoxNo ratings yet
- Drugs For PLAB 2 - Cheat SheetDocument3 pagesDrugs For PLAB 2 - Cheat SheetLiviousoeNo ratings yet
- FarmakologiDocument7 pagesFarmakologiNicole NgoNo ratings yet
- Drug Study of TBDocument7 pagesDrug Study of TBMarc AntonioNo ratings yet
- PrescribingDocument2 pagesPrescribingPei Xing KwekNo ratings yet
- CASE 1 GBS ADULT PHARMACISTs CARE PLANDocument3 pagesCASE 1 GBS ADULT PHARMACISTs CARE PLANquina mjNo ratings yet
- Neoplsma Uro, FK Ums 2010Document130 pagesNeoplsma Uro, FK Ums 2010nursidiq10No ratings yet
- Obat-Obat NefrotoksikDocument43 pagesObat-Obat Nefrotoksiknursidiq10100% (1)
- Obat-Obat Pada Syndrome Nefrotik (SN/NS)Document34 pagesObat-Obat Pada Syndrome Nefrotik (SN/NS)nursidiq10No ratings yet
- Obat IskDocument6 pagesObat Isknursidiq10No ratings yet
- 1 Penyakit GinjalDocument43 pages1 Penyakit Ginjalnursidiq10No ratings yet
- Obat-Obat NefrotoksikDocument43 pagesObat-Obat Nefrotoksiknursidiq10100% (1)
- Obat IskDocument6 pagesObat Isknursidiq10No ratings yet
- Bab I II III IV V Aan Edited OKDocument4 pagesBab I II III IV V Aan Edited OKnursidiq10No ratings yet
- 1 PDFDocument22 pages1 PDFnursidiq10No ratings yet
- Jurnal DBDDocument9 pagesJurnal DBDnursidiq10No ratings yet
- Jurnal DBDDocument9 pagesJurnal DBDnursidiq10No ratings yet
- DHFDocument9 pagesDHFMuhammad Nur SidiqNo ratings yet
- Daftar PustakaDocument1 pageDaftar Pustakanursidiq10No ratings yet
- Rhomboid Flap For Pilonidal Sinus - Our ExperienceDocument5 pagesRhomboid Flap For Pilonidal Sinus - Our ExperienceKhalidHussainNo ratings yet
- A Decade of Dementia Care Training Learning Needs PDFDocument10 pagesA Decade of Dementia Care Training Learning Needs PDFYovana Pachón PovedaNo ratings yet
- Muet EssaysDocument29 pagesMuet EssaysBabasChongNo ratings yet
- The Daily Tar Heel For April 12, 2016Document8 pagesThe Daily Tar Heel For April 12, 2016The Daily Tar HeelNo ratings yet
- Assignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Document3 pagesAssignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Hafshah AgustinaNo ratings yet
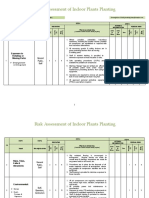
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- (OSHPD 1, 2, 3 & 4) See Sections 404.0 Through 418.0. (SFM) Air Filters Shall Comply With All Requirements ofDocument0 pages(OSHPD 1, 2, 3 & 4) See Sections 404.0 Through 418.0. (SFM) Air Filters Shall Comply With All Requirements ofOanh NguyenNo ratings yet
- Telescopic Handler Student ManualDocument41 pagesTelescopic Handler Student ManualingcalderonNo ratings yet
- Vyankatesh City-IIDocument17 pagesVyankatesh City-IIapi-27095887No ratings yet
- Johnson ReportDocument10 pagesJohnson ReportHarihar SharmaNo ratings yet
- Liver Vascular Anatomy - A RefresherDocument10 pagesLiver Vascular Anatomy - A Refresherilham nugrohoNo ratings yet
- Flux Cored Arc Welding NC IIDocument73 pagesFlux Cored Arc Welding NC IIAJ AcuñaNo ratings yet
- Introducing Behavioural Markers of Non-Technical Skills in Oil and Gas OperationsDocument24 pagesIntroducing Behavioural Markers of Non-Technical Skills in Oil and Gas OperationsMarutpal MukherjeeNo ratings yet
- Good Practice Review - 8 - Revised2 PDFDocument323 pagesGood Practice Review - 8 - Revised2 PDFsteppevosNo ratings yet
- Jawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthDocument18 pagesJawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthIvan OliveiraNo ratings yet
- Alcohol Abuse Nicholas Black Professor Patton 7/6/2017Document9 pagesAlcohol Abuse Nicholas Black Professor Patton 7/6/2017iuibuibNo ratings yet
- Budget of Works in Grade 7 Health: S.Y. 2019 - 2020 Quarter Topics Objectives Activites No. of HoursDocument1 pageBudget of Works in Grade 7 Health: S.Y. 2019 - 2020 Quarter Topics Objectives Activites No. of HoursRichard MarquezNo ratings yet
- CrimPro Cases (Rule 116)Document45 pagesCrimPro Cases (Rule 116)elvinperiaNo ratings yet
- Suplemento 1Document56 pagesSuplemento 1Dessirhe LaraNo ratings yet
- Three Biological Humors (The Tridoshas-Vata, Pitta and Kapha) and Their Role in Human SystemDocument45 pagesThree Biological Humors (The Tridoshas-Vata, Pitta and Kapha) and Their Role in Human SystemPrashanthNo ratings yet
- Plasma Metanephrine Test: Patient Information FactsheetDocument2 pagesPlasma Metanephrine Test: Patient Information FactsheetDamigart PremiumNo ratings yet
- Antifoam Oh Conz - GHS EngDocument11 pagesAntifoam Oh Conz - GHS EngOUSMAN SEIDNo ratings yet
- Postural DrainageDocument7 pagesPostural DrainagemohtishimNo ratings yet
- Peduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Document11 pagesPeduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Grace BrigondoNo ratings yet
- HaloperidolDocument1 pageHaloperidolSalma AKNo ratings yet
- AIA IHS Clinics With TCM - Generic (120613)Document43 pagesAIA IHS Clinics With TCM - Generic (120613)junkaiiiNo ratings yet
- CXC Csec English A June 2015 p1Document16 pagesCXC Csec English A June 2015 p1Rihanna Johnson100% (1)
- Uworld RationalesDocument2 pagesUworld RationalesMelissa Sapp67% (3)
- YMCA Program Guide - 2016Document44 pagesYMCA Program Guide - 2016Pickens County YMCANo ratings yet
- Spring Term Core A Formative AssessmentDocument9 pagesSpring Term Core A Formative Assessmentdiscord.tazzNo ratings yet