You might also like
- Prometric Questions OrthoDocument13 pagesPrometric Questions OrthoFaisal Mushtaq67% (12)
- Obstetric Hemorrhage Checklist: Safe Motherhood InitiativeDocument2 pagesObstetric Hemorrhage Checklist: Safe Motherhood InitiativejefeNo ratings yet
- Comply With Infection Prevention and Control Policies and ProceduresDocument42 pagesComply With Infection Prevention and Control Policies and Procedurespavan0% (1)
- Penatalaksanan Intensif Pasien Penyakit Tropik Berat Di ICUDocument24 pagesPenatalaksanan Intensif Pasien Penyakit Tropik Berat Di ICUMichael WijayaNo ratings yet
- Guidelines and Protocols Of: Diabetes EmergenciesDocument36 pagesGuidelines and Protocols Of: Diabetes Emergenciesyassen hassanNo ratings yet
- Internal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiDocument209 pagesInternal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiSilvi Qiro'atul AiniNo ratings yet
- Pharmacology Report: Dengue Shock Syndrome OutlineDocument3 pagesPharmacology Report: Dengue Shock Syndrome OutlineLizbeth Aura CebrianNo ratings yet
- DR. LEONARD-Fluid Dengue TangerangDocument30 pagesDR. LEONARD-Fluid Dengue TangerangHerry KongkoNo ratings yet
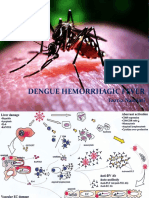
- Dengue Hemorrhagic Fever: Fazria NasriatiDocument19 pagesDengue Hemorrhagic Fever: Fazria NasriatiElsa KarinasariNo ratings yet
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungDocument47 pagesKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiNo ratings yet
- Penatalaksanaan DSSDocument29 pagesPenatalaksanaan DSSTugas HeinzNo ratings yet
- Blood TransfusionDocument8 pagesBlood TransfusionmagizhchijoyceNo ratings yet
- Management Dengue HXDocument6 pagesManagement Dengue HXMalshika JayatissaNo ratings yet
- Farma StrokeDocument37 pagesFarma StrokeDAHLIANo ratings yet
- Canine Blood Component TableDocument1 pageCanine Blood Component TableTrifan PatriciaNo ratings yet
- Approach To ShockDocument40 pagesApproach To ShockDivesh NaiduNo ratings yet
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel0% (1)
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)ghellersNo ratings yet
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel100% (2)
- Adult: Diabetic Emergencies: Care Protocol and ChartDocument4 pagesAdult: Diabetic Emergencies: Care Protocol and ChartvladhdNo ratings yet
- Rational Use of Safe BloodDocument22 pagesRational Use of Safe Bloodkamnasharma0907No ratings yet
- Do'S and Don'Ts For DoctorsDocument4 pagesDo'S and Don'Ts For DoctorsTalha ENo ratings yet
- Emergency GuidelinesDocument11 pagesEmergency GuidelineswinstonappsNo ratings yet
- Fluid ManagementDocument34 pagesFluid ManagementPradeep VunnamNo ratings yet
- Fluid Therapy in Surgical PatientsDocument20 pagesFluid Therapy in Surgical PatientsTehniyath MariyamNo ratings yet
- Fluid Therapy in Paediatrics - RevisedDocument5 pagesFluid Therapy in Paediatrics - RevisedJehangir AllamNo ratings yet
- Malignant Hyperthermia PDFDocument5 pagesMalignant Hyperthermia PDFKyla Barrera TabungarNo ratings yet
- Homologous Blood Trasfusion Practice ShortsDocument23 pagesHomologous Blood Trasfusion Practice ShortsdrprasadingleyNo ratings yet
- Management Protocol of Septic Shock: DiagnosisDocument3 pagesManagement Protocol of Septic Shock: Diagnosissky nutsNo ratings yet
- Assessment and Concept Map Care Plan For Critical Care PatientDocument11 pagesAssessment and Concept Map Care Plan For Critical Care Patientapi-604551723No ratings yet
- Golden Period Septic ChildDocument32 pagesGolden Period Septic ChildcallNo ratings yet
- Diabetic Ketoacidosis PathwayDocument22 pagesDiabetic Ketoacidosis PathwaySri Nath100% (1)
- Fluid Resuscitation in SepsisDocument68 pagesFluid Resuscitation in SepsisRonald Ariyanto WiradirnataNo ratings yet
- What Is Fluid Therapy?Document42 pagesWhat Is Fluid Therapy?Mirel YdianNo ratings yet
- ShockDocument27 pagesShockyashmodi5555No ratings yet
- Fluid ManagementDocument10 pagesFluid ManagementdradaadNo ratings yet
- Early Symptoms: Insidious Increase in Polydipsia and PolyuriaDocument3 pagesEarly Symptoms: Insidious Increase in Polydipsia and Polyuriabes3rkerNo ratings yet
- Massive Transfusion ProtocolDocument1 pageMassive Transfusion ProtocoldraymanhussiennotionNo ratings yet
- Blood and Blood Products: Presenter: TAN LI LIAN Supervisor: DR AMINDocument15 pagesBlood and Blood Products: Presenter: TAN LI LIAN Supervisor: DR AMINNur Amin MuhammadNo ratings yet
- Prevention and Medical Management of Uterine Atony: by Cheong Lu Jeat, Laow Yee Kean Supervised by DR MunisDocument17 pagesPrevention and Medical Management of Uterine Atony: by Cheong Lu Jeat, Laow Yee Kean Supervised by DR MunisCatherine PingNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- NullDocument58 pagesNullElteyb Nor eldaimNo ratings yet
- MGT of D KetoacidosisDocument5 pagesMGT of D Ketoacidosisshabatat2002No ratings yet
- Dengue Fever Management - Pediatrics SeminarDocument106 pagesDengue Fever Management - Pediatrics SeminarAimhigh_PPMNo ratings yet
- Dengue FinalDocument24 pagesDengue FinalManju ManjunathNo ratings yet
- BWH Hyperglycemia GuidelinesDocument7 pagesBWH Hyperglycemia Guidelinespmahesh107100% (1)
- NICU Drugs GuideDocument49 pagesNICU Drugs GuideArhanNo ratings yet
- West Midlands Regional Training Package For Safe Blood Transfusion PracticeDocument20 pagesWest Midlands Regional Training Package For Safe Blood Transfusion PracticeekramsNo ratings yet
- What Is Fluid Therapy?Document42 pagesWhat Is Fluid Therapy?Mirel YdianNo ratings yet
- Patient Units Severe Sepsis Screening ToolDocument2 pagesPatient Units Severe Sepsis Screening ToolArnelli HutagalungNo ratings yet
- ATOTW 136 Major Haemorrhage Part 1 2009Document6 pagesATOTW 136 Major Haemorrhage Part 1 2009viaereaNo ratings yet
- DKA Protocol TGDocument11 pagesDKA Protocol TGabelNo ratings yet
- Electrolyte Prescribe Gline AdultDocument2 pagesElectrolyte Prescribe Gline AdultMirelaNo ratings yet
- Hypokalaemia PDFDocument2 pagesHypokalaemia PDFjenna1213No ratings yet
- Hypokalaemia PDFDocument2 pagesHypokalaemia PDFRisaNo ratings yet
- Guideline For The Management of Hypokalaemia in Adults: Signs & SymptomsDocument2 pagesGuideline For The Management of Hypokalaemia in Adults: Signs & SymptomsmuzakiNo ratings yet
- Hypokalaemia PDFDocument2 pagesHypokalaemia PDFIulia RoxanaNo ratings yet
- Hypokalaemia PDFDocument2 pagesHypokalaemia PDFManuela KarinaaNo ratings yet
- Blood and Blood Product (F)Document50 pagesBlood and Blood Product (F)bharat singhNo ratings yet
- L 13 High Dose Methotrexate High Grade NHL Cns ProphylaxisDocument6 pagesL 13 High Dose Methotrexate High Grade NHL Cns ProphylaxisHanin MaharNo ratings yet
- Renal Guide and Charts: AlbuminDocument16 pagesRenal Guide and Charts: AlbuminYaima JimenezNo ratings yet
- Hughes 2015Document5 pagesHughes 2015edelinNo ratings yet
- Induction of MMP-9 Mediated Gelatinolytic Activity in Human Monocytic Cells by Cell Wall Components of Mycobacterium TuberculosisDocument14 pagesInduction of MMP-9 Mediated Gelatinolytic Activity in Human Monocytic Cells by Cell Wall Components of Mycobacterium TuberculosisedelinNo ratings yet
- Life and Death in The Granuloma: Immunopathology of TuberculosisDocument9 pagesLife and Death in The Granuloma: Immunopathology of TuberculosisedelinNo ratings yet
- Blink Reflex: AnatomyDocument5 pagesBlink Reflex: AnatomyedelinNo ratings yet
- Salahuddin2007 PDFDocument6 pagesSalahuddin2007 PDFedelinNo ratings yet
- Kim 2009Document7 pagesKim 2009edelinNo ratings yet
- Matrix Metalloproteinase-8 (MMP-8) Is The Major Collagenase in Human DentinDocument7 pagesMatrix Metalloproteinase-8 (MMP-8) Is The Major Collagenase in Human DentinedelinNo ratings yet
- Angiogenic Factors in The Pathogenesis and Pathophysiology of Preeclampsia A Mini ReviewDocument7 pagesAngiogenic Factors in The Pathogenesis and Pathophysiology of Preeclampsia A Mini ReviewedelinNo ratings yet
- Day Case Vaginal Pomeroy Tubectomy A Simplified TechniqueDocument11 pagesDay Case Vaginal Pomeroy Tubectomy A Simplified TechniqueedelinNo ratings yet
- Man Nello 2005Document15 pagesMan Nello 2005edelinNo ratings yet
- Jtgga 17 1 16Document5 pagesJtgga 17 1 16edelinNo ratings yet
- Research: Uterine Artery Doppler Study in Second Trimester of PregnancyDocument8 pagesResearch: Uterine Artery Doppler Study in Second Trimester of PregnancyedelinNo ratings yet
- Thomas 2007Document11 pagesThomas 2007edelinNo ratings yet
- NIH Public Access: Author ManuscriptDocument10 pagesNIH Public Access: Author ManuscriptedelinNo ratings yet
- A Novel Human-Specific Soluble Vascular Endothelial Growth Factor Receptor 1Document21 pagesA Novel Human-Specific Soluble Vascular Endothelial Growth Factor Receptor 1edelinNo ratings yet
- 7 Hyperthyroidism Nursing Care Plan (NCP)Document1 page7 Hyperthyroidism Nursing Care Plan (NCP)Apol PenNo ratings yet
- Material Safety Data Sheet: Section 1 - IdentificationDocument4 pagesMaterial Safety Data Sheet: Section 1 - Identificationmohamed AdelNo ratings yet
- Gabra 2018Document5 pagesGabra 2018Titis Retno Sawitri SawitriNo ratings yet
- MS Sas 5Document5 pagesMS Sas 5rereNo ratings yet
- Diagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseDocument1 pageDiagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseLauraNo ratings yet
- A Narrative Evaluation of Homeopathic Relevance in Treating Autoimmune Diseases, Including Rheumatoid Arthritis, With Rubrics and JustificationsDocument11 pagesA Narrative Evaluation of Homeopathic Relevance in Treating Autoimmune Diseases, Including Rheumatoid Arthritis, With Rubrics and JustificationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CHN Module 1Document34 pagesCHN Module 1Don Maur ValeteNo ratings yet
- Igm Arc ChemDocument8 pagesIgm Arc Chembassam alharaziNo ratings yet
- DR Manish Soni: MD (Gold Medalist), IADVL Fellow (AIIMS, New Delhi) EDocument135 pagesDR Manish Soni: MD (Gold Medalist), IADVL Fellow (AIIMS, New Delhi) ESahib PathanNo ratings yet
- Health of Newly Arrived Immigrants in Canada and The United StatesDocument10 pagesHealth of Newly Arrived Immigrants in Canada and The United StatesRafael AlfradiqueNo ratings yet
- What's Missing GameDocument25 pagesWhat's Missing GameJohn Paolo OcampoNo ratings yet
- Group 3 Title DefenseDocument10 pagesGroup 3 Title Defensejamokbaisas297No ratings yet
- DR Ashraf Gift To DR AlvaroDocument16 pagesDR Ashraf Gift To DR AlvaroAhmed Saleh100% (1)
- Lesson Plan Stress ManagemenntDocument5 pagesLesson Plan Stress ManagemenntJose I. Petras IIINo ratings yet
- Appendix B-Acceptable AcronymsDocument11 pagesAppendix B-Acceptable AcronymsKimberly SolisNo ratings yet
- Funda Lec MidtermsDocument13 pagesFunda Lec MidtermsCharisse CaydanNo ratings yet
- FHSISDocument31 pagesFHSISNezer SorianoNo ratings yet
- 0221 Thermo Purification Efficiency Ebook 8Document8 pages0221 Thermo Purification Efficiency Ebook 8liondredNo ratings yet
- (MICROBIO) Liver Fluke NewDocument100 pages(MICROBIO) Liver Fluke NewMadhu MithaNo ratings yet
- How Orthomolecular Medicine Can Help: Contributed by Dr. Abram HofferDocument11 pagesHow Orthomolecular Medicine Can Help: Contributed by Dr. Abram HofferWilliam AckermannNo ratings yet
- Uptodate: Chronic Kidney DiseaseDocument13 pagesUptodate: Chronic Kidney DiseaseAtiqah ShahNo ratings yet
- Fatty Liver: Millions of Liver Suffer in SilenceDocument40 pagesFatty Liver: Millions of Liver Suffer in SilenceTafsir arefinNo ratings yet
- SorilDocument10 pagesSorilelieser toding mendilaNo ratings yet
- Medical Abbreviations - Taber's Medical DictionaryDocument15 pagesMedical Abbreviations - Taber's Medical DictionaryRose Antonette BenitoNo ratings yet
- Teflon: Created and Presented By: Dulvan.DDocument16 pagesTeflon: Created and Presented By: Dulvan.DDulvan Devnaka Senaratne100% (1)
- ANZCOR Guideline 13.4 - Airway Management and Mask Ventilation of The NewbornDocument18 pagesANZCOR Guideline 13.4 - Airway Management and Mask Ventilation of The NewbornEssam HassanNo ratings yet
- RE6210E Errata SheetsDocument10 pagesRE6210E Errata Sheetsamandinewodzich1211No ratings yet
- Handwashing Glo Germ Lab 1 2 PDFDocument4 pagesHandwashing Glo Germ Lab 1 2 PDFSummer StonesNo ratings yet