You might also like
- DR. LEONARD-Fluid Dengue TangerangDocument30 pagesDR. LEONARD-Fluid Dengue TangerangHerry KongkoNo ratings yet
- Penatalaksanaan DSSDocument29 pagesPenatalaksanaan DSSTugas HeinzNo ratings yet
- Penatalaksanan Intensif Pasien Dengan Penyakit Tropik Berat Di ICUDocument24 pagesPenatalaksanan Intensif Pasien Dengan Penyakit Tropik Berat Di ICUedelinNo ratings yet
- Materi Pratugas Interenship 2017Document27 pagesMateri Pratugas Interenship 2017Angga MahayasaNo ratings yet
- Penatalaksanan Intensif Pasien Penyakit Tropik Berat Di ICUDocument24 pagesPenatalaksanan Intensif Pasien Penyakit Tropik Berat Di ICUMichael WijayaNo ratings yet
- Diagnosis and Management of DHF and DssDocument24 pagesDiagnosis and Management of DHF and DssRini Airin AwaluddinNo ratings yet
- Condition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockDocument4 pagesCondition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockJohnPaulOliverosNo ratings yet
- Guideline For The Management of Adults Patients With DKA or HHSDocument3 pagesGuideline For The Management of Adults Patients With DKA or HHSJonard GiloNo ratings yet
- Guidelines and Protocols Of: Diabetes EmergenciesDocument36 pagesGuidelines and Protocols Of: Diabetes Emergenciesyassen hassanNo ratings yet
- 3.4 Summary - ShockDocument1 page3.4 Summary - ShockPedro Clement nkom bakwaphNo ratings yet
- Dengue Fever MX Protocol Summary Updated (Dengue1)Document11 pagesDengue Fever MX Protocol Summary Updated (Dengue1)ashokarathnasingheNo ratings yet
- EPALS DKA Flowchart Jan 23 V4Document1 pageEPALS DKA Flowchart Jan 23 V4Miguel BaiaNo ratings yet
- Adult: Diabetic Emergencies: Care Protocol and ChartDocument4 pagesAdult: Diabetic Emergencies: Care Protocol and ChartvladhdNo ratings yet
- DR Leonar, DENGUE PIN PAPDI 2019Document51 pagesDR Leonar, DENGUE PIN PAPDI 2019Yuni Purnama SariNo ratings yet
- TWU Anesthesia Cheat SheetDocument2 pagesTWU Anesthesia Cheat Sheetinvading_jam7582100% (5)
- 3-Management of DF-DHF2018Document36 pages3-Management of DF-DHF2018koengphearom9No ratings yet
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungDocument47 pagesKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiNo ratings yet
- Fluid Therapy in Paediatrics - RevisedDocument5 pagesFluid Therapy in Paediatrics - RevisedJehangir AllamNo ratings yet
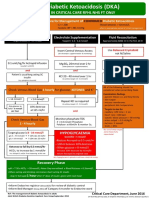
- Adult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyDocument1 pageAdult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyJung Bahadur SinghNo ratings yet
- Algorithm For Fluid Management in Decompensated ShockDocument1 pageAlgorithm For Fluid Management in Decompensated Shocklieynna4996No ratings yet
- Principles of Management of DKADocument4 pagesPrinciples of Management of DKAHassen Kavi IsseNo ratings yet
- Renal Guide and Charts: AlbuminDocument16 pagesRenal Guide and Charts: AlbuminYaima JimenezNo ratings yet
- Drugrenaladjustment 12052565Document18 pagesDrugrenaladjustment 12052565jirat iyarapongNo ratings yet
- BWH Hyperglycemia GuidelinesDocument7 pagesBWH Hyperglycemia Guidelinespmahesh107100% (1)
- Fluid and Electrolytes ManagementDocument21 pagesFluid and Electrolytes ManagementRasYa DINo ratings yet
- Dka CalculatorDocument1 pageDka CalculatordelfiaNo ratings yet
- DKACalculatorDocument1 pageDKACalculatorRitch BassNo ratings yet
- 1 FluidsDocument17 pages1 FluidsMae CalunsagNo ratings yet
- 2014 SHC ABX Dosing GuideDocument4 pages2014 SHC ABX Dosing GuideisnaeniNo ratings yet
- Urgentno Zbrinjavanje Dehidracije Kod Dece EngDocument43 pagesUrgentno Zbrinjavanje Dehidracije Kod Dece EngMirko BelanNo ratings yet
- Start Isotonic Crystalloid 10-20mml/kg/hr For 1 HourDocument2 pagesStart Isotonic Crystalloid 10-20mml/kg/hr For 1 HourMayasumita Wijayana05No ratings yet
- Early Symptoms: Insidious Increase in Polydipsia and PolyuriaDocument3 pagesEarly Symptoms: Insidious Increase in Polydipsia and Polyuriabes3rkerNo ratings yet
- Assessment and Concept Map Care Plan For Critical Care PatientDocument11 pagesAssessment and Concept Map Care Plan For Critical Care Patientapi-604551723No ratings yet
- Dehydration - PedsCase - v9Document1 pageDehydration - PedsCase - v9Chinenye ModestaNo ratings yet
- InfusDocument29 pagesInfusfauzanNo ratings yet
- Pharmacology Report: Dengue Shock Syndrome OutlineDocument3 pagesPharmacology Report: Dengue Shock Syndrome OutlineLizbeth Aura CebrianNo ratings yet
- DengueDocument19 pagesDengueCieAciCiiNo ratings yet
- DKA Guidelines Version 4.0 28 Dec 2016FINALDocument4 pagesDKA Guidelines Version 4.0 28 Dec 2016FINALbenNo ratings yet
- 2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Document63 pages2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Andy DazNo ratings yet
- 2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Document63 pages2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Andy DazNo ratings yet
- Replacement CairanDocument26 pagesReplacement CairanLuthfi HakimNo ratings yet
- Map DkaDocument1 pageMap DkaSH PrageethNo ratings yet
- Peds DrugsDocument79 pagesPeds DrugsmodakaneeketgmNo ratings yet
- Antidote Card: Orogastric Lavage With Large Bore TubeDocument2 pagesAntidote Card: Orogastric Lavage With Large Bore Tubemataro13No ratings yet
- Dka-Hhs Topic DiscussionDocument2 pagesDka-Hhs Topic Discussionapi-648401824No ratings yet
- 2499 Rapid Hospital ProtocolDocument2 pages2499 Rapid Hospital ProtocolMohamad Nofal Abu HasanNo ratings yet
- Neonatal HypertensionDocument21 pagesNeonatal HypertensionMuhammad Ammar Abdul WahabNo ratings yet
- Treatment of Acute Hypokalaemia in AdultsDocument4 pagesTreatment of Acute Hypokalaemia in AdultsEmaNo ratings yet
- SAM Dehydration Algorithm - 29042021Document2 pagesSAM Dehydration Algorithm - 29042021samarmojeebNo ratings yet
- Stanford Health Care Antimicrobial Dosing Reference GuideDocument7 pagesStanford Health Care Antimicrobial Dosing Reference GuideKarl Martin PinedaNo ratings yet
- Drug Study: Antacid GI: Belching, GastricDocument3 pagesDrug Study: Antacid GI: Belching, GastricJhon Jade PalagtiwNo ratings yet
- Notes ImDocument5 pagesNotes Imsharmee sarmientaNo ratings yet
- Diabetic Ketoacidosis Dka Hyperglycemic Hyperosmolar State Hhs Adult PDFDocument4 pagesDiabetic Ketoacidosis Dka Hyperglycemic Hyperosmolar State Hhs Adult PDFyayaNo ratings yet
- Fluid and Electrolytes 1.Document26 pagesFluid and Electrolytes 1.Ethan LimNo ratings yet
- CalciumchannelalgorithmDocument1 pageCalciumchannelalgorithmLind YLNo ratings yet
- BCCH Diabetic Ketoacidosis Protocol Toolkit: Endocrinology & Diabetes UnitDocument16 pagesBCCH Diabetic Ketoacidosis Protocol Toolkit: Endocrinology & Diabetes UnitaseelNo ratings yet
- SHC ABX Dosing GuideDocument7 pagesSHC ABX Dosing GuideDanielVillaNo ratings yet
- Revised DKA 2015 PDFDocument6 pagesRevised DKA 2015 PDFDr AhmedNo ratings yet
- Fluids and Electrolyte PediatricsDocument41 pagesFluids and Electrolyte PediatricsYusron BishryNo ratings yet
- Q. With RationalDocument102 pagesQ. With RationalDr-Sanjay SinghaniaNo ratings yet
- What Is Coronary Bypass Surgery?: HeartDocument2 pagesWhat Is Coronary Bypass Surgery?: HeartSebastian BujorNo ratings yet
- Acute Phase ProteinsDocument380 pagesAcute Phase ProteinsRogerio CansiNo ratings yet
- Anatomy - Kidney'sDocument18 pagesAnatomy - Kidney'sOlivia MorrisonNo ratings yet
- Anatomy of LungsDocument4 pagesAnatomy of Lungs31 PASION, ROCHELLE C.No ratings yet
- Unit-I-IMTH-III (Osmosis, Types of Solution & Plasmolysis) PDFDocument47 pagesUnit-I-IMTH-III (Osmosis, Types of Solution & Plasmolysis) PDFanuksha aroraNo ratings yet
- Acpuncture Points & Cinese NamesDocument4 pagesAcpuncture Points & Cinese NamesVivekanandanvrNo ratings yet
- Marfan Does Not Mean Martian - 0Document28 pagesMarfan Does Not Mean Martian - 0Anonymous S5bG7pNo ratings yet
- Pet ScanDocument40 pagesPet ScanAkhilesh KhobragadeNo ratings yet
- Musculo-Skeletal TraumaDocument48 pagesMusculo-Skeletal TraumaNagashree VNo ratings yet
- Sleep 7Document11 pagesSleep 7Dyah Ayu KusumawarddhaniNo ratings yet
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 66Document15 pagesMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 66sarasjunkNo ratings yet
- Oral CavityDocument65 pagesOral Cavityugwuokeprince4No ratings yet
- Valsalva ManeuverDocument9 pagesValsalva ManeuverRina YulianaNo ratings yet
- Introduction To Chiral or Optical IsomersDocument3 pagesIntroduction To Chiral or Optical IsomersSeepana Dayakar100% (1)
- PAPER (ENG) - Pseudodysphagia Due To Omohyoid Muscle SyndromeDocument6 pagesPAPER (ENG) - Pseudodysphagia Due To Omohyoid Muscle SyndromeAldo Hip NaranjoNo ratings yet
- Anat MuscleDocument164 pagesAnat Musclejohn delaNo ratings yet
- Bradycardia GuidelineDocument2 pagesBradycardia Guidelinekannan73dr100% (1)
- Cell Organelles Webquest Day 2 With Notes Filled inDocument3 pagesCell Organelles Webquest Day 2 With Notes Filled inJustin TisNo ratings yet
- Clinical Laboratory Hematology 3rd Edition Mckenzie Test BankDocument35 pagesClinical Laboratory Hematology 3rd Edition Mckenzie Test Bankgeincupola.06zi100% (28)
- 1111111111111111111111111111111Document7 pages1111111111111111111111111111111Andrei Jose V. LayeseNo ratings yet
- Accessory Glands of The GITDocument12 pagesAccessory Glands of The GITSheena PasionNo ratings yet
- June 2010 (v1) QP - Paper 2 CIE Biology IGCSEDocument16 pagesJune 2010 (v1) QP - Paper 2 CIE Biology IGCSESriyashas KalluriNo ratings yet
- Approach To Cyanosis in A NeonateDocument12 pagesApproach To Cyanosis in A NeonateXerxyllXyreaneLinaoNo ratings yet
- Protein Energy Malnutrition (PEM)Document39 pagesProtein Energy Malnutrition (PEM)CLEMENT100% (3)
- Physiology of DigestionDocument23 pagesPhysiology of DigestionLàXsun ShrèsthàNo ratings yet
- REFERAT Lumbar Compression FractureDocument25 pagesREFERAT Lumbar Compression FractureTaufik Ghockil ZlaluwNo ratings yet
- Common Drugs and Antidotes: Antidote Indication Mode of ActionDocument2 pagesCommon Drugs and Antidotes: Antidote Indication Mode of ActionPiny CesarNo ratings yet
- ThalassemiaDocument59 pagesThalassemiaAndhika Hadi Wirawan0% (1)
- A Case Presentation On Burns: Brokenshire Integrated Health Ministries Incorporated Department of General SurgeryDocument42 pagesA Case Presentation On Burns: Brokenshire Integrated Health Ministries Incorporated Department of General SurgeryCharles Gerard B. BeluanNo ratings yet