You might also like
- MAD Magazine 001Document36 pagesMAD Magazine 001ClarkcoffeyNo ratings yet
- New American Paintings - December-January, 2019Document180 pagesNew American Paintings - December-January, 2019Fabio Nagual100% (1)
- Top Nursing Skills, Procedures and Normal ValuesDocument25 pagesTop Nursing Skills, Procedures and Normal ValuesericNo ratings yet
- Ajuste IAC and TPSDocument17 pagesAjuste IAC and TPSLuis Ignacio SilvaNo ratings yet
- Cheat Sheet (Draft)Document3 pagesCheat Sheet (Draft)bonziebuddyNo ratings yet
- 24 HR History 2Document2 pages24 HR History 2Arjun KatariaNo ratings yet
- Cellulitis Oral Case PresDocument48 pagesCellulitis Oral Case PresLet BorlagdanNo ratings yet
- 2 0CommDiseaseIMPTVisionDocument3 pages2 0CommDiseaseIMPTVisionAndrea Patricia DaquialNo ratings yet
- Anesthesia Drug DosageDocument13 pagesAnesthesia Drug DosageLuqman HakimNo ratings yet
- Development Length ACI 318-14 v2.0Document5 pagesDevelopment Length ACI 318-14 v2.0Raymund Dale P. BallenasNo ratings yet
- Ames Perception ExperimentsDocument108 pagesAmes Perception ExperimentsMichael RoseNo ratings yet
- B757-200 MPDDocument393 pagesB757-200 MPDSebastian Rendon100% (3)
- Clinical Abstract TEMPLATEDocument3 pagesClinical Abstract TEMPLATEDiannesa April GolosindaNo ratings yet
- CPG PneumoniaDocument31 pagesCPG PneumoniaJo Anne100% (3)
- IM Cardiology Samplex All-In - LDocument35 pagesIM Cardiology Samplex All-In - LDeepbluexNo ratings yet
- Mp1 Type 1 ManualDocument69 pagesMp1 Type 1 ManualJerryNo ratings yet
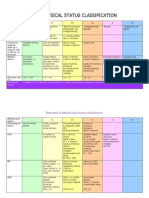
- ASA physical status classification guideDocument3 pagesASA physical status classification guideMelisa Malik0% (1)
- 2.seismic Coefficient CalculationDocument14 pages2.seismic Coefficient CalculationVenkat PalliNo ratings yet
- Renal Replacement TherapyDocument11 pagesRenal Replacement TherapyZahra AlaradiNo ratings yet
- DL Throughput Improvement with Aperiodic CQI ReportingDocument10 pagesDL Throughput Improvement with Aperiodic CQI ReportingAqeel HasanNo ratings yet
- Surgery Case AppendicitisDocument30 pagesSurgery Case AppendicitisSarahNo ratings yet
- Management of Upper GI BleedingDocument55 pagesManagement of Upper GI BleedingNatnaelNo ratings yet
- Renal Lab Tests ExplainedDocument67 pagesRenal Lab Tests ExplainedRjDNo ratings yet
- Physician Order Sheet Format GuideDocument9 pagesPhysician Order Sheet Format GuideRoland Philip GoNo ratings yet
- Case Presentation: NeurologyDocument19 pagesCase Presentation: NeurologySydrex SarmientoNo ratings yet
- Clinical Evaluation of DehydrationDocument5 pagesClinical Evaluation of DehydrationEricka Lyn Arenas MonzonNo ratings yet
- Hypoxia and CyanosisDocument33 pagesHypoxia and CyanosisRamlah IbrahimNo ratings yet
- C191W003 Control Bleeding and Hypovolemic ShockDocument51 pagesC191W003 Control Bleeding and Hypovolemic ShockEmad Hussien Haj-AbdullaNo ratings yet
- 46-Year-Old Man With Abnormal Lipid ProfileDocument3 pages46-Year-Old Man With Abnormal Lipid ProfileCamiiliita Fernández La TorreNo ratings yet
- RhabdomyolysisDocument2 pagesRhabdomyolysisintrovoyz041No ratings yet
- Aquino Typhoid Fever Case PresentationDocument9 pagesAquino Typhoid Fever Case PresentationCalingalan Hussin CaluangNo ratings yet
- BWH Hyperglycemia GuidelinesDocument7 pagesBWH Hyperglycemia Guidelinespmahesh107100% (1)
- Bronchial Asthma: West Visayas State University Medical Center - Department of PediatricsDocument9 pagesBronchial Asthma: West Visayas State University Medical Center - Department of PediatricsPGI Miayo, StephenNo ratings yet
- Sheehan SyndromeDocument6 pagesSheehan SyndromeArvie TagnongNo ratings yet
- Case Study 2Document4 pagesCase Study 2api-2451636590% (1)
- Pre-Op Case Protocol #4Document2 pagesPre-Op Case Protocol #4IC BNo ratings yet
- Burn Injury PathophysiologyDocument1 pageBurn Injury PathophysiologyMonique Ann DanoyNo ratings yet
- Junior Intern NotesDocument3 pagesJunior Intern NotesTin SumangaNo ratings yet
- Guide to assessment and management of acute gastroenteritisDocument2 pagesGuide to assessment and management of acute gastroenteritisMaya LarasNo ratings yet
- Child's Abdominal Pain Admitting ConferenceDocument24 pagesChild's Abdominal Pain Admitting ConferenceRaul MangrobangNo ratings yet
- Case 2 and 3 Q1Document3 pagesCase 2 and 3 Q1Jeffrey Ramos0% (1)
- RevalidaDocument5 pagesRevalidaHawkins FletcherNo ratings yet
- Approach to Hypertension ManagementDocument11 pagesApproach to Hypertension ManagementNoreenNo ratings yet
- RabiesDocument10 pagesRabiesWinda LiraNo ratings yet
- Bleeding DisordersDocument24 pagesBleeding Disorderskholoud220No ratings yet
- IM AdconDocument28 pagesIM AdconCla SantosNo ratings yet
- CAD - EBM September 2020 EditionDocument17 pagesCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiNo ratings yet
- Cardiology Case 1Document2 pagesCardiology Case 1vil62650% (2)
- Massive Ventral Hernia Case StudyDocument7 pagesMassive Ventral Hernia Case StudysugisweNo ratings yet
- Acute Lymphoblastic LeukemiaDocument25 pagesAcute Lymphoblastic Leukemiaapi-396564080No ratings yet
- Approximate Equivalents:: 0.100 Gmn. 1.00 GMDocument8 pagesApproximate Equivalents:: 0.100 Gmn. 1.00 GMakane ryuNo ratings yet
- Peptic Ulcer DiseaseDocument14 pagesPeptic Ulcer DiseasePernel Jose Alam MicuboNo ratings yet
- Final GIT Case PresentationDocument53 pagesFinal GIT Case PresentationRovan100% (1)
- Fever of Unknown OriginDocument26 pagesFever of Unknown OriginFiona Yona Sitali100% (1)
- Dams - DVT (New)Document48 pagesDams - DVT (New)Msd KishorNo ratings yet
- PulmoconDocument64 pagesPulmoconapi-3704562100% (1)
- Concept Map Meningitis TheoryDocument3 pagesConcept Map Meningitis TheoryMia AuliaNo ratings yet
- REYE SYNDROME: ACUTE ENCEPHALOPATHY AND FATTY LIVERDocument10 pagesREYE SYNDROME: ACUTE ENCEPHALOPATHY AND FATTY LIVERDanil KhairulNo ratings yet
- Progress NoteDocument3 pagesProgress NoteHaji JawaroNo ratings yet
- Ugib &lgibDocument41 pagesUgib &lgibDawex IsraelNo ratings yet
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDocument25 pagesClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiNo ratings yet
- Case PCAPDocument2 pagesCase PCAPNina Anne ParacadNo ratings yet
- HypertensionDocument6 pagesHypertensionTj Kevin P-DoctorNo ratings yet
- Approach to Dyslipidemia Based on 2015 CPGDocument26 pagesApproach to Dyslipidemia Based on 2015 CPGRenzy SalumbreNo ratings yet
- Kawasaki Disease DiagnosisDocument5 pagesKawasaki Disease DiagnosisFranz SalazarNo ratings yet
- Difficulty Breathing Case ReportDocument6 pagesDifficulty Breathing Case ReportRaian SuyuNo ratings yet
- CVD Bleed Case StudyDocument25 pagesCVD Bleed Case StudyMargaret Jenaw JenawNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Worksheet - Word Tracing - HibiscusDocument1 pageWorksheet - Word Tracing - HibiscusCatherine PingNo ratings yet
- Worksheet - Word Tracing - Jalur GemilangDocument1 pageWorksheet - Word Tracing - Jalur GemilangCatherine PingNo ratings yet
- Worksheet - Cut - Paste - MalaysiaDocument1 pageWorksheet - Cut - Paste - MalaysiaCatherine PingNo ratings yet
- 3b (II) Dice Game InstructionDocument1 page3b (II) Dice Game InstructionCatherine PingNo ratings yet
- Worksheet - Word Tracing - MalaysiaDocument1 pageWorksheet - Word Tracing - MalaysiaCatherine PingNo ratings yet
- Thanks For Downloading This Awesome Activity!: Visit For More Super Simple Learning Ideas!Document6 pagesThanks For Downloading This Awesome Activity!: Visit For More Super Simple Learning Ideas!Catherine PingNo ratings yet
- Massive PPHDocument7 pagesMassive PPHCatherine PingNo ratings yet
- +i-Think Programme MapsDocument2 pages+i-Think Programme MapsNicholas HenryNo ratings yet
- My Five Senses: Match The Pictures To The Correct SensesDocument1 pageMy Five Senses: Match The Pictures To The Correct Sensesjekay acayNo ratings yet
- 0510 FridayDocument2 pages0510 FridayCatherine PingNo ratings yet
- Kemahiran Abad 21 2012Document23 pagesKemahiran Abad 21 2012abey_whereNo ratings yet
- Thanks For Downloading This Awesome Activity!: GraphicsDocument5 pagesThanks For Downloading This Awesome Activity!: GraphicsCatherine PingNo ratings yet
- Values and Ethics in The PDFDocument32 pagesValues and Ethics in The PDFCatherine PingNo ratings yet
- Acog Hemorragia PostpartoDocument9 pagesAcog Hemorragia PostpartoHollman オルマンNo ratings yet
- 1-10 PuzzleDocument2 pages1-10 PuzzleCatherine PingNo ratings yet
- Taklimat Umum KSSRDocument38 pagesTaklimat Umum KSSRwanis_75No ratings yet
- Hemorragia Obstetrica 4Document6 pagesHemorragia Obstetrica 4Evelyn Ramirez MamaniNo ratings yet
- Nursery Rhyme Head Shoulders Knees and ToesDocument1 pageNursery Rhyme Head Shoulders Knees and ToesCatherine PingNo ratings yet
- Counseling HbeDocument9 pagesCounseling HbeCatherine PingNo ratings yet
- Carta Organisasi Kelas Jadual Waktu KelasDocument2 pagesCarta Organisasi Kelas Jadual Waktu KelasCatherine PingNo ratings yet
- Quite Books PDFDocument28 pagesQuite Books PDFCatherine PingNo ratings yet
- Creative Leadership by GeraldDocument57 pagesCreative Leadership by GeraldCatherine PingNo ratings yet
- 1307 FriDocument1 page1307 FriCatherine PingNo ratings yet
- Jadual TugasanDocument5 pagesJadual TugasanCatherine PingNo ratings yet
- I-Think Maps WSMDocument7 pagesI-Think Maps WSMAnonymous UypCttWNo ratings yet
- Nine Events of Instruction: BehavioristDocument3 pagesNine Events of Instruction: BehavioristCatherine PingNo ratings yet
- Critique CMADocument10 pagesCritique CMAannyss elleNo ratings yet
- Interpreting Standard DeviationsDocument8 pagesInterpreting Standard DeviationsCatherine PingNo ratings yet
- GlossaryDocument3 pagesGlossaryThảo ĐỗNo ratings yet
- Incremental and Newton Methods Lab ReportDocument10 pagesIncremental and Newton Methods Lab ReportAbde RrahimNo ratings yet
- Group 1 STEM 12 2P SIP FINALDocument17 pagesGroup 1 STEM 12 2P SIP FINALFhing FhingNo ratings yet
- Chapter 1 - Quiz 2 Form A: A. B. C. D. E. F. G. H. I. J. K. L. M. N. O. P. 1. 2. 3. 4. 5. 6. 7. 8Document2 pagesChapter 1 - Quiz 2 Form A: A. B. C. D. E. F. G. H. I. J. K. L. M. N. O. P. 1. 2. 3. 4. 5. 6. 7. 8Olalekan Oyekunle0% (1)
- Frequency-Domain Analysis of Discrete-Time Signals and SystemsDocument31 pagesFrequency-Domain Analysis of Discrete-Time Signals and SystemsSwatiSharmaNo ratings yet
- LinearDocument46 pagesLinearSheikh Riasat100% (1)
- Revisiting The Irish Royal Sites: Susan A. JohnstonDocument7 pagesRevisiting The Irish Royal Sites: Susan A. JohnstonJacek RomanowNo ratings yet
- Bitterness Compounds in Coffee Brew Measured by Analytical Instruments and Taste Sensing SystemDocument34 pagesBitterness Compounds in Coffee Brew Measured by Analytical Instruments and Taste Sensing SystemSolisNo ratings yet
- Pacemaker 180508042454Document86 pagesPacemaker 180508042454padmaNo ratings yet
- IVOZI Pronunciation SoundDocument2 pagesIVOZI Pronunciation Soundlorena13ntNo ratings yet
- 3D Bioprinting From The Micrometer To Millimete 2017 Current Opinion in BiomDocument7 pages3D Bioprinting From The Micrometer To Millimete 2017 Current Opinion in Biomrrm77No ratings yet
- Mushroom Umami Taste EvaluationDocument10 pagesMushroom Umami Taste EvaluationMaryam HanifNo ratings yet
- Atoms & Ions Worksheet 1 /63: Atomic Number and Mass NumberDocument4 pagesAtoms & Ions Worksheet 1 /63: Atomic Number and Mass Numbercate christineNo ratings yet
- Vammika Sutta - Mahasi SayadawDocument108 pagesVammika Sutta - Mahasi SayadawtravelbootsNo ratings yet
- A Perspective in Accelerated Orthodontics With Aligner Treatment 2017 Seminars in OrthodonticsDocument7 pagesA Perspective in Accelerated Orthodontics With Aligner Treatment 2017 Seminars in Orthodonticsdruzair007No ratings yet
- Assignment 1 (Total Marks: 70) EEE 323: Power System IIDocument2 pagesAssignment 1 (Total Marks: 70) EEE 323: Power System IIShahriar SauravNo ratings yet
- Unit 1.Pptx Autosaved 5bf659481837fDocument39 pagesUnit 1.Pptx Autosaved 5bf659481837fBernadith Manaday BabaloNo ratings yet
- 5 Commandments of DatingDocument8 pages5 Commandments of DatingBariki MwasagaNo ratings yet
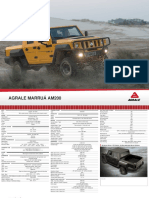
- Off Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Document2 pagesOff Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Victor SilvaNo ratings yet
- DSBV87ALP Two-Stage Differential Pressure Control Valve SpecsDocument2 pagesDSBV87ALP Two-Stage Differential Pressure Control Valve SpecsadrianioantomaNo ratings yet
- PHYS205 Matlab Lab TasksDocument4 pagesPHYS205 Matlab Lab TasksjacobNo ratings yet
- SEO-Optimized Title for Quantitative Techniques for Business-II Exam DocumentDocument4 pagesSEO-Optimized Title for Quantitative Techniques for Business-II Exam DocumentEthan WillsNo ratings yet