You might also like
- Anatomy and PhysiologyDocument87 pagesAnatomy and PhysiologyMenaka ShanthiNo ratings yet
- Surface Anatomy, Position and Radiologic AnatomyDocument12 pagesSurface Anatomy, Position and Radiologic AnatomyBill DiazNo ratings yet
- Naveen K PT 12/03/2020Document57 pagesNaveen K PT 12/03/2020Naveen Kumar100% (1)
- The Human Organism: Anatomy & Physiology Lecture - Chapter 1Document7 pagesThe Human Organism: Anatomy & Physiology Lecture - Chapter 1christine delgadoNo ratings yet
- 1-5 Occlusion in Removable Partial ProsthodonticsDocument5 pages1-5 Occlusion in Removable Partial ProsthodonticsIlse100% (1)
- FRCSOrthExam Education Viva Topics1Document20 pagesFRCSOrthExam Education Viva Topics1ts8166No ratings yet
- Mrcs Anatomy McqsDocument92 pagesMrcs Anatomy McqsJohn M. Hemsworth100% (1)
- Medical Imaging: Translating 2 Dimensional Mri Scans of the Human Forearm into 3 Dimensional Dielectric PhantomsFrom EverandMedical Imaging: Translating 2 Dimensional Mri Scans of the Human Forearm into 3 Dimensional Dielectric PhantomsNo ratings yet
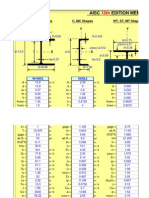
- AISC 13.0 Properties ViewerDocument18 pagesAISC 13.0 Properties ViewerramilianNo ratings yet
- Exstore NotesDocument7 pagesExstore NotesAlvaro ToledoNo ratings yet
- A Case Report of Human Skeletal Remains Performed Tameshi-GiriDocument10 pagesA Case Report of Human Skeletal Remains Performed Tameshi-GiriCostantino Isononami Dojo BrandozziNo ratings yet
- Biscevic Evoluta EvolventaDocument6 pagesBiscevic Evoluta EvolventaDino PracicNo ratings yet
- Morphometric Changes in The Heights and Anteroposterior Diameters of The Lumbar Intervertebral Discs With Age - Amono-Kuofi Et Al. 1991 PDFDocument10 pagesMorphometric Changes in The Heights and Anteroposterior Diameters of The Lumbar Intervertebral Discs With Age - Amono-Kuofi Et Al. 1991 PDFMohammad KaramNo ratings yet
- The Association Between Lumbar Rib and Lumbosacral Transitional VertebraeDocument14 pagesThe Association Between Lumbar Rib and Lumbosacral Transitional VertebraeAnGBalNo ratings yet
- Shoulder Impingement Syndromes: Folco RossiDocument7 pagesShoulder Impingement Syndromes: Folco RossiAnanta MiaNo ratings yet
- MRI of The Posterolateral Corner Injury: A Concise ReviewDocument6 pagesMRI of The Posterolateral Corner Injury: A Concise ReviewIntanNo ratings yet
- Ijcmsr 312 v1Document7 pagesIjcmsr 312 v1AshliiqueNo ratings yet
- Comparative Study of Mechanical Stresses in Human Limb BonesDocument9 pagesComparative Study of Mechanical Stresses in Human Limb BonesTejas krishnakanthNo ratings yet
- Avascular Necrosis OF THE Femoral HeadDocument5 pagesAvascular Necrosis OF THE Femoral HeadAnees HojaNo ratings yet
- Paper Submission ISBS FinalDocument4 pagesPaper Submission ISBS FinalbachmanndominicNo ratings yet
- Management of Femoral Shaft Fractures: M. V. Neumann, N. P. Südkamp, P. C. StrohmDocument11 pagesManagement of Femoral Shaft Fractures: M. V. Neumann, N. P. Südkamp, P. C. StrohmRema AmerNo ratings yet
- Color PDFDocument38 pagesColor PDFel_mekawyNo ratings yet
- Mri Evaluation of Shoulder Joint: Normal Anatomy & Pathological Finding A Pictorial Essay and ReviewDocument9 pagesMri Evaluation of Shoulder Joint: Normal Anatomy & Pathological Finding A Pictorial Essay and ReviewIqhe Harsono SyastrowinotoNo ratings yet
- Biomechanical Analysis of Free Shooting in BasketballDocument10 pagesBiomechanical Analysis of Free Shooting in BasketballRaj PinkyNo ratings yet
- Columna LumbarDocument54 pagesColumna LumbarSamantha AriasNo ratings yet
- Go Gle Go Gle: List of The Human Skeleton in Forensic MedicintDocument11 pagesGo Gle Go Gle: List of The Human Skeleton in Forensic Medicintt80uNo ratings yet
- Atwood 1971 JPD Reduction of Residual Ridges A Major Oral Disease EntityDocument19 pagesAtwood 1971 JPD Reduction of Residual Ridges A Major Oral Disease EntitySolano Barboza Carlos GaelNo ratings yet
- Morphometric Analysis of The Inferior Vena Cava Related To Lumbar Vertebra and The Aortic BifurcationDocument8 pagesMorphometric Analysis of The Inferior Vena Cava Related To Lumbar Vertebra and The Aortic Bifurcation17091974No ratings yet
- Tendon Del Subescapular - Sistema de Clasificación - AnatomíaDocument7 pagesTendon Del Subescapular - Sistema de Clasificación - AnatomíajesusglezctNo ratings yet
- Analise Morfologica Da Faceta Costal Da Vertebra ToracicaDocument11 pagesAnalise Morfologica Da Faceta Costal Da Vertebra ToracicaPaula Duarte MarquesNo ratings yet
- Studies of Body Movements in Kendo Men StrikesDocument7 pagesStudies of Body Movements in Kendo Men StrikesidrologiaeambienteNo ratings yet
- Vector (Butterfly) Diagrams For Osteoarthritic Gait A Preliminary Report - KhodadadehDocument5 pagesVector (Butterfly) Diagrams For Osteoarthritic Gait A Preliminary Report - KhodadadehpetcudanielNo ratings yet
- DiagnosDocument40 pagesDiagnosRamon Alberto Portillo MedinaNo ratings yet
- Anatomy of Plexus Branchialis PDFDocument24 pagesAnatomy of Plexus Branchialis PDFGemantri veyonda ZikryNo ratings yet
- Act A 1990Document5 pagesAct A 1990Elvedin TrakićNo ratings yet
- Rotator Cuff Tear Arthropathy: Pathophysiology, Imaging Characteristics, and Treatment OptionsDocument10 pagesRotator Cuff Tear Arthropathy: Pathophysiology, Imaging Characteristics, and Treatment OptionsYuni AngrianiNo ratings yet
- Free Full Text: Biomechanical Analysis of Snatch Movement and Vertical Jump: Similarities and DifferencesDocument6 pagesFree Full Text: Biomechanical Analysis of Snatch Movement and Vertical Jump: Similarities and DifferencesHari SetiawanNo ratings yet
- The Aetiology of Subacromial Impingement Syndrome: Key Words 458Document12 pagesThe Aetiology of Subacromial Impingement Syndrome: Key Words 458Spiros TsoukanelisNo ratings yet
- A Crescent-Shaped Juxtafacet Cyst As A Rare Cause of High Thoracic Myelopathy With Partial Brown-Séquard's SyndromeDocument3 pagesA Crescent-Shaped Juxtafacet Cyst As A Rare Cause of High Thoracic Myelopathy With Partial Brown-Séquard's Syndromeg9dhczvdjxNo ratings yet
- Assimetria Mandibular 3DDocument8 pagesAssimetria Mandibular 3DJúnior MarotoNo ratings yet
- Electromechanical Behaviour of Human Muscles in Vertical JumpsDocument9 pagesElectromechanical Behaviour of Human Muscles in Vertical JumpsAugusto Felipe Benavides MejiasNo ratings yet
- MDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewDocument9 pagesMDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewcalinmariusNo ratings yet
- Axial Rotation Component of Thoracic Scoliosis - Stokes1989Document7 pagesAxial Rotation Component of Thoracic Scoliosis - Stokes1989Mohammad KaramNo ratings yet
- 2011 Epidemiology of Muscle Injuries in Professional Football (Soccer)Document7 pages2011 Epidemiology of Muscle Injuries in Professional Football (Soccer)Physio AcademyNo ratings yet
- 3D Atlas of Lumbar SpineDocument16 pages3D Atlas of Lumbar Spinehari vijayNo ratings yet
- M55 Case StudyDocument100 pagesM55 Case StudyLexi RobertsNo ratings yet
- Changes in Articular Eminence Inclination During The Craniofacial Growth PeriodDocument7 pagesChanges in Articular Eminence Inclination During The Craniofacial Growth PeriodDentist HereNo ratings yet
- ScoliosisDocument11 pagesScoliosisFatenNo ratings yet
- Sectional Anatomy of Spine (Cervical, Dorsal, and Lumbo-Sacral)Document68 pagesSectional Anatomy of Spine (Cervical, Dorsal, and Lumbo-Sacral)tendi AndriansayahNo ratings yet
- Imaging of Osteonecrosis of The Femoral HeadDocument28 pagesImaging of Osteonecrosis of The Femoral Headgreg_enricoNo ratings yet
- PathomechanicsDocument8 pagesPathomechanicsMike B AndersonNo ratings yet
- The Elbow - Radio Graphic Imaging Pearls and PitfallsDocument25 pagesThe Elbow - Radio Graphic Imaging Pearls and PitfallsDarko IllusionNo ratings yet
- Morphometry of Lower Lumbar Vertebrae As Seen On CT Scans:: Newly Recognized CharacteristicsDocument9 pagesMorphometry of Lower Lumbar Vertebrae As Seen On CT Scans:: Newly Recognized CharacteristicsDayXena ApahtNo ratings yet
- Jurnal VertebraDocument10 pagesJurnal VertebraGeorge Herland PradiktaNo ratings yet
- Paprosky Classification of Acetabular Bone LossDocument6 pagesPaprosky Classification of Acetabular Bone Lossamine roujdiNo ratings yet
- Studies of Body Movements in Kendo Men OruchanDocument9 pagesStudies of Body Movements in Kendo Men OruchanidrologiaeambienteNo ratings yet
- Europeanjournalof Radiologyopen: Longitudinal Stress Fracture of The Femur: A Rare PresentationDocument4 pagesEuropeanjournalof Radiologyopen: Longitudinal Stress Fracture of The Femur: A Rare PresentationYusfaIndahNo ratings yet
- La C K of Bo N e S T I F F N e S S S T R e N G T H Contribution To Osteoarthritis - Evidence For Primary Role of Cartilage DamageDocument4 pagesLa C K of Bo N e S T I F F N e S S S T R e N G T H Contribution To Osteoarthritis - Evidence For Primary Role of Cartilage DamageSTAF OSCENo ratings yet
- Crack Effect On Human Femur Bone Under Axial LoadDocument8 pagesCrack Effect On Human Femur Bone Under Axial Loadالراصد طبيNo ratings yet
- LutterDocument17 pagesLutterVL3 MXXNNo ratings yet
- Description of The Sagittal Alignment of The Degenerative Human SpineDocument8 pagesDescription of The Sagittal Alignment of The Degenerative Human SpineKenNo ratings yet
- Normal Range of Motion of The Hip Knee and Ankle Joints in Male Subjects 30 40 Years of AgeDocument5 pagesNormal Range of Motion of The Hip Knee and Ankle Joints in Male Subjects 30 40 Years of AgeAbdul RazzaqNo ratings yet
- Jurding SkoliosisDocument20 pagesJurding SkoliosisAndiniNo ratings yet
- Finite Element Analysis of Human Femur BoneDocument14 pagesFinite Element Analysis of Human Femur BoneAreez KhanNo ratings yet
- PEARL Classification Rotator CuffDocument4 pagesPEARL Classification Rotator CuffAntonio PNo ratings yet
- Architectural Pattern of Animals: Animals According To Body CavityDocument6 pagesArchitectural Pattern of Animals: Animals According To Body CavityMaisonette MichNo ratings yet
- A Practical Guide For Performing Arthrography Under Fluoroscopic or Ultrasound GuidanceDocument10 pagesA Practical Guide For Performing Arthrography Under Fluoroscopic or Ultrasound GuidanceSnehanshNo ratings yet
- Atlas of Approaches in Neurosurgery - J.FischerDocument7 pagesAtlas of Approaches in Neurosurgery - J.FischerZdravko HeinrichNo ratings yet
- Introduction ProjectDocument66 pagesIntroduction ProjectYsnet PremNo ratings yet
- Examples of Superior Examples of Inferior: PlanesDocument2 pagesExamples of Superior Examples of Inferior: PlanesDorothy MaglenteNo ratings yet
- 04 New Obstetric ExaminationDocument44 pages04 New Obstetric Examinationfranny90No ratings yet
- Anatomy Trains DVDDocument3 pagesAnatomy Trains DVDdrprasantNo ratings yet
- Haplochromis Electra: Studies On The Family CichlidaeDocument5 pagesHaplochromis Electra: Studies On The Family CichlidaeCenk Sururi KarabulutNo ratings yet
- About Flying LizardDocument11 pagesAbout Flying LizardRiswan Hanafyah HarahapNo ratings yet
- 02 - Biomechanical Analysis of Sit-To-stand Movement in Normal and Obese SubjectsDocument6 pages02 - Biomechanical Analysis of Sit-To-stand Movement in Normal and Obese SubjectsCristian HuequelefNo ratings yet
- APS Acupuncture Points and Meridians IDocument18 pagesAPS Acupuncture Points and Meridians Ipassagerx007No ratings yet
- Introduction To Anatomy and Physiology Part 2Document6 pagesIntroduction To Anatomy and Physiology Part 2Abby Claire SomeraNo ratings yet
- Equine Veterinary Journal - 2014 - MacKinnon - Analysis of Stress Fractures Associated With Lameness in Thoroughbred FlatDocument6 pagesEquine Veterinary Journal - 2014 - MacKinnon - Analysis of Stress Fractures Associated With Lameness in Thoroughbred FlatMARIA PAZ MORENO CONTRERASNo ratings yet
- LWBK836 Ch111 p1194-1208Document15 pagesLWBK836 Ch111 p1194-1208metasoniko81No ratings yet
- Multiple AbrasionDocument10 pagesMultiple AbrasionChristian Ureta0% (1)
- Module 1 PATHFit1 Chapters 1 3Document46 pagesModule 1 PATHFit1 Chapters 1 3naomimarielleNo ratings yet
- Superficial and Deep Facial Anatomy and Its Implications For RhytidectomyDocument9 pagesSuperficial and Deep Facial Anatomy and Its Implications For Rhytidectomyjaviers45No ratings yet
- Chapter 1: Introduction To Anatomy and Physiology NotesDocument6 pagesChapter 1: Introduction To Anatomy and Physiology Notesapi-305436791No ratings yet
- RAC KMC Mock Test Final YearDocument7 pagesRAC KMC Mock Test Final YearYoung FlameNo ratings yet
- Project Work in Fish DiversityDocument29 pagesProject Work in Fish DiversityBisari Mikhu63% (8)
- Heron R.F Titarsole Konsulen: Dr. Wijaya J. Chendra, SP - OTDocument48 pagesHeron R.F Titarsole Konsulen: Dr. Wijaya J. Chendra, SP - OTAnton ChristianNo ratings yet
- Unit # 01 Intoduction To A & P Insta - Husain.z.kmuDocument33 pagesUnit # 01 Intoduction To A & P Insta - Husain.z.kmuMuhammad RiazNo ratings yet
- United States Patent (10) Patent No.: US 9.255,753 B2Document31 pagesUnited States Patent (10) Patent No.: US 9.255,753 B2Anonymous VNu3ODGavNo ratings yet