You might also like
- Root Cause Analysis Handbook: A Guide to Efficient and Effective Incident InvestigationFrom EverandRoot Cause Analysis Handbook: A Guide to Efficient and Effective Incident InvestigationNo ratings yet
- Root Cause Analysis Course OverviewDocument102 pagesRoot Cause Analysis Course Overviewwaran87100% (1)
- Training On Root Cause Analysis / Problem Solving TechniquesDocument66 pagesTraining On Root Cause Analysis / Problem Solving TechniquesDINESH SHARMANo ratings yet
- 5 Why TrainingDocument38 pages5 Why Trainingliviu_din_codru100% (8)
- Root Cause TemplateDocument19 pagesRoot Cause TemplateFiroz Khan100% (3)
- Root Cause Analysis by MonicaDocument19 pagesRoot Cause Analysis by MonicaMonica B100% (1)
- Root Cause AnalysisDocument9 pagesRoot Cause AnalysisAl Engg100% (9)
- 5 Why Root Cause AnalysisDocument1 page5 Why Root Cause AnalysisSinan İcik100% (1)
- Root Cause Analysis (RCA) TrainingDocument153 pagesRoot Cause Analysis (RCA) TrainingSolha89% (9)
- Root Cause AnalysisDocument47 pagesRoot Cause Analysiskapindra100% (8)
- Root Cause Analysis PresentationDocument37 pagesRoot Cause Analysis PresentationucheonixNo ratings yet
- Cause - Effect and Root - Cause AnalysisDocument25 pagesCause - Effect and Root - Cause AnalysiszawadzahinNo ratings yet
- Root Cause AnalysisDocument105 pagesRoot Cause AnalysisJay R Ballon100% (3)
- Root Cause Analysis ToolsDocument31 pagesRoot Cause Analysis ToolsDanielaGarcia100% (2)
- 5 Why AnalysisDocument55 pages5 Why AnalysisHarshit Sharma100% (1)
- Root Causes AnalisysDocument33 pagesRoot Causes Analisysandrés_donossoNo ratings yet
- Root Cause Analysis Tools: A Complete GuideDocument22 pagesRoot Cause Analysis Tools: A Complete Guidejmpbarros100% (4)
- Root Cause Analysis - ToolDocument11 pagesRoot Cause Analysis - ToolFouzan SoniwalaNo ratings yet
- RCA TrainingDocument15 pagesRCA TrainingfelicityNo ratings yet
- Root Cause MapDocument2 pagesRoot Cause Mapamevaluaciones100% (1)
- Root Cause Analysis MPM1-GlDocument39 pagesRoot Cause Analysis MPM1-GlJunaid KhanNo ratings yet
- Root Cause Analysis FormsDocument58 pagesRoot Cause Analysis Formsapi-3701688100% (4)
- Root Cause AnalysisDocument16 pagesRoot Cause AnalysisPat TejNo ratings yet
- AI Root Cause AnalysisDocument27 pagesAI Root Cause AnalysisAsuman100% (1)
- Root Cause AnalysisDocument21 pagesRoot Cause Analysischngan432257% (7)
- Root Cause AnalysisDocument28 pagesRoot Cause Analysisaftabseven2No ratings yet
- Root Cause Analysis PaperDocument6 pagesRoot Cause Analysis Paperapi-272448190100% (1)
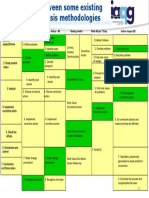
- Root Cause Analysis Methodologies IAQGDocument1 pageRoot Cause Analysis Methodologies IAQGAldo100% (1)
- Root Cause AnalysisDocument56 pagesRoot Cause AnalysisDhana Raju100% (1)
- The Basics of Root Cause AnalysisDocument20 pagesThe Basics of Root Cause Analysismauriciojj100% (1)
- Root Cause Analysis - VVGGG Cases PDFDocument54 pagesRoot Cause Analysis - VVGGG Cases PDFnorthbride2008No ratings yet
- Root Cause AnalysisDocument1 pageRoot Cause AnalysisSick LoveNo ratings yet
- 5 Whys TrainingDocument14 pages5 Whys TrainingPanch BNo ratings yet
- Root Cause Analysis TemplateDocument4 pagesRoot Cause Analysis Templatekareem34560% (1)
- Root Cause Analysis (RCA) & 8-D Team Oriented Problem SolvingDocument197 pagesRoot Cause Analysis (RCA) & 8-D Team Oriented Problem SolvingAhamed Shareef S ANo ratings yet
- Root Cause AnalysisDocument16 pagesRoot Cause AnalysisBryan NguyenNo ratings yet
- RCA Framework TemplateDocument9 pagesRCA Framework TemplateDevi ChintyaNo ratings yet
- Understanding RCA MethodsDocument21 pagesUnderstanding RCA MethodsLammie Sing Yew Lam100% (2)
- Root Cause AnalysisDocument5 pagesRoot Cause Analysistamara_002150% (2)
- 5 WHYs ROOT CAUSE ANALYSIS TEMPLATEDocument2 pages5 WHYs ROOT CAUSE ANALYSIS TEMPLATEAjiwuriNo ratings yet
- Root Cause Analysis Report Form InsightsDocument7 pagesRoot Cause Analysis Report Form Insightsbenaoumeur benounaNo ratings yet
- 5 WHYs Root Cause AnalysisDocument2 pages5 WHYs Root Cause AnalysisDwi SurantoNo ratings yet
- Root Cause AnalysisDocument18 pagesRoot Cause AnalysisJohn Brix Balisteros100% (3)
- Root Cause Analysis Corrective ActionDocument12 pagesRoot Cause Analysis Corrective ActionAbdulrahman Alkhowaiter100% (2)
- Root Cause AnalysisDocument12 pagesRoot Cause Analysisosalp internationalNo ratings yet
- Root Cause Analysis for Safety IncidentsDocument27 pagesRoot Cause Analysis for Safety IncidentsKARTHIK NAIKARNo ratings yet
- 5 WhysDocument2 pages5 WhysJim Adams100% (1)
- Root Cause Analysis (RCA)Document20 pagesRoot Cause Analysis (RCA)Shieradel Jimenez100% (1)
- Nexteer's 3L5Y supplier issue analysisDocument1 pageNexteer's 3L5Y supplier issue analysisvandukul100% (1)
- Root Cause AnalysisDocument105 pagesRoot Cause AnalysisPunjabi Stars Update100% (1)
- Root Cause AnalysisDocument46 pagesRoot Cause AnalysisK60 THẠCH THÁI HÂNNo ratings yet
- Chapter 16 - Problem Solving and Decision Making ProcessDocument20 pagesChapter 16 - Problem Solving and Decision Making ProcessAnanda RiskiNo ratings yet
- Root Cause & Corrective Action Corrective Action (RCCA) (RCCA)Document37 pagesRoot Cause & Corrective Action Corrective Action (RCCA) (RCCA)Bisma Masood100% (1)
- Rca PPT Lean ManagementDocument43 pagesRca PPT Lean ManagementPreeti BahetiNo ratings yet
- 8d Problem SolvingDocument117 pages8d Problem SolvingChan Kok Khan100% (1)
- Lect 9 - Lean Sixsigma - Part - IIIDocument46 pagesLect 9 - Lean Sixsigma - Part - IIIlangzayNo ratings yet
- Chap 001Document19 pagesChap 001Sag-e-AttarNo ratings yet
- Chap 001Document19 pagesChap 001Muhammad FarhanNo ratings yet
- 8D Problem Solving Excel WorksheetDocument6 pages8D Problem Solving Excel WorksheetecdtcenterNo ratings yet
- 8D:: Problem Solving Worksheet: Tracking Number: Customer Number: Response Due DateDocument8 pages8D:: Problem Solving Worksheet: Tracking Number: Customer Number: Response Due DatePawel WeilNo ratings yet
- MGT 6203 - Sri - M5 - Treatment Effects v042919Document21 pagesMGT 6203 - Sri - M5 - Treatment Effects v042919lexleong9610No ratings yet
- Sesi 3C - Konsep Penyebab Penyakit IiDocument100 pagesSesi 3C - Konsep Penyebab Penyakit IidewiNo ratings yet
- Anstey - The Science of Nature in The Seventeenth CenturyDocument251 pagesAnstey - The Science of Nature in The Seventeenth CenturyArcanaNo ratings yet
- Seria V - 1 2016Document368 pagesSeria V - 1 2016Joaquin CosavalenteNo ratings yet
- Surviving your Dissertation MethodsDocument28 pagesSurviving your Dissertation Methodsmlist1No ratings yet
- BHP Activity 2019 U9-6 Understanding The Causes of World War I StudentDocument3 pagesBHP Activity 2019 U9-6 Understanding The Causes of World War I StudentPallavi SharmaNo ratings yet
- Service Marketing Word FileDocument31 pagesService Marketing Word FileSachin MethreeNo ratings yet
- Simona Rich - 11 Universal LawsDocument38 pagesSimona Rich - 11 Universal LawsBrindusa Balasa100% (1)
- Patterns of DevelopmentDocument4 pagesPatterns of DevelopmentEllen Obsina100% (1)
- Metaphysics IntroductionDocument3 pagesMetaphysics IntroductionZairen Mae Piloneo100% (1)
- Notes in Theories of Crime CausationDocument79 pagesNotes in Theories of Crime CausationRaiza LopezNo ratings yet
- Presentation by Ishtiaq Ahmad (IUB)Document22 pagesPresentation by Ishtiaq Ahmad (IUB)ishtiaqlodhranNo ratings yet
- Accident Causation Theories and ConceptDocument4 pagesAccident Causation Theories and ConceptShayne Aira AnggongNo ratings yet
- Risk Quantification For New Product Design and Development in A Concurrent Engineering EnvironmentDocument4 pagesRisk Quantification For New Product Design and Development in A Concurrent Engineering Environmentsachin_choudhary_5No ratings yet
- Koslowski - Theory and Evidence. The Development of Scientific ReasoningDocument297 pagesKoslowski - Theory and Evidence. The Development of Scientific ReasoningJohnnie Z. DrakeNo ratings yet
- Rosato - The Flawed Logic of Democratic Peace TheoryDocument19 pagesRosato - The Flawed Logic of Democratic Peace Theorymartin_kunNo ratings yet
- Research questions & answersDocument2 pagesResearch questions & answersJayan NairNo ratings yet
- William Dunn Policy AnalysisDocument65 pagesWilliam Dunn Policy AnalysisKarl Wyne NatividadNo ratings yet
- A Scientific Approach To Determining Root Cause NOTESDocument118 pagesA Scientific Approach To Determining Root Cause NOTESSTEVEN DELAHUNTYNo ratings yet
- Fish Bone DiagramDocument10 pagesFish Bone Diagramghafoorian_khoshgovar1488No ratings yet
- Teaching - NLP and Pupil Motivation PDFDocument9 pagesTeaching - NLP and Pupil Motivation PDFgoodguy_swk100% (2)
- Experimental PsychologyDocument8 pagesExperimental PsychologykylamadelcNo ratings yet
- Why Is Social Psychology Important To Us?Document7 pagesWhy Is Social Psychology Important To Us?Tasneem ShabbirNo ratings yet
- CRM For Cabin CrewDocument15 pagesCRM For Cabin CrewCristian Ciobanu100% (1)
- Self-Determination in HumansDocument16 pagesSelf-Determination in HumansLawrence CahooneNo ratings yet
- 7 Quality Control Tools (Basic) : Srinivas R KhodeDocument22 pages7 Quality Control Tools (Basic) : Srinivas R Khodemeteora13580% (5)
- CBC Events Management NC IIIDocument102 pagesCBC Events Management NC IIINhoj Eiram100% (1)
- Lecture 8: Risk Management: Software Development Project Management (CSC4125)Document51 pagesLecture 8: Risk Management: Software Development Project Management (CSC4125)rohanNo ratings yet
- IMK Documentation ModelDocument75 pagesIMK Documentation ModelMarlon Barrios Solano0% (1)
- Hypothesis Between Quantitative and Qualitative ResearchDocument10 pagesHypothesis Between Quantitative and Qualitative ResearchmaimamaiyNo ratings yet