You might also like
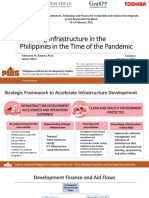
- Session 4.3 - Financing Infrastructure in The Philippines in The Time of The PandemicDocument17 pagesSession 4.3 - Financing Infrastructure in The Philippines in The Time of The PandemicAdila ArdissaNo ratings yet
- Chapter 5 Ensuring People Centered Clean and Efficient GovernanceDocument15 pagesChapter 5 Ensuring People Centered Clean and Efficient GovernancePeter ParedesNo ratings yet
- Detailed Feasibility Report: Animal Feed UnitDocument56 pagesDetailed Feasibility Report: Animal Feed UnitSam Di FerralivaNo ratings yet
- MPCIF Guideline 1Document53 pagesMPCIF Guideline 1Raaz DhakalNo ratings yet
- KEY FEATURES OF THE 2023-24 BUDGET-06 February 2023-CompressedDocument16 pagesKEY FEATURES OF THE 2023-24 BUDGET-06 February 2023-Compressedfiercesasha8808No ratings yet
- Chapter 8 Expanding Economic Opportunities in Agriculture Forestry and FisheriesDocument35 pagesChapter 8 Expanding Economic Opportunities in Agriculture Forestry and FisheriesPeter ParedesNo ratings yet
- Indonesia Infrastructure Development: Ministry of Finance The Republic of IndonesiaDocument16 pagesIndonesia Infrastructure Development: Ministry of Finance The Republic of IndonesiaHarristio AdamNo ratings yet
- PMNP 1Document33 pagesPMNP 1Yang ObreroNo ratings yet
- Double-Glazed ReportDocument72 pagesDouble-Glazed Reportshidik hossenNo ratings yet
- Roadmap Development and Reinforcement For Information Technology-Based Joint Funding Services 2023-2028Document84 pagesRoadmap Development and Reinforcement For Information Technology-Based Joint Funding Services 2023-2028balqisNo ratings yet
- Detailed Project Report: "Government User Network" For Service Delivery at Village LevelDocument164 pagesDetailed Project Report: "Government User Network" For Service Delivery at Village Levelsagar cherryNo ratings yet
- Agro Product ReportDocument75 pagesAgro Product ReportNaumanNo ratings yet
- BPLS Automation Planning and Implementation GuideDocument74 pagesBPLS Automation Planning and Implementation Guidebong goNo ratings yet
- #2 CROP Secretariats Engagement Session FY2023Document188 pages#2 CROP Secretariats Engagement Session FY2023Mohd SyahmiNo ratings yet
- Guidelines For ICT-RTMDocument48 pagesGuidelines For ICT-RTMSubheshPatelNo ratings yet
- Updated 2017 2022 PIP As Input To FY 2020 Budget Preparation Chapter 16 As of 12april19Document1 pageUpdated 2017 2022 PIP As Input To FY 2020 Budget Preparation Chapter 16 As of 12april19detailsNo ratings yet
- Milk PowderDocument68 pagesMilk Powderruthchell manatad100% (1)
- Kartika Wirjoatmodjo - Mandiri (GR)Document16 pagesKartika Wirjoatmodjo - Mandiri (GR)data informasi gambirNo ratings yet
- List of Priority Programs and Projects in The 2017-2022 Public Investment Programs (PIP) Chapter 15: Ensuring Sound Macroeconomic PolicyDocument2 pagesList of Priority Programs and Projects in The 2017-2022 Public Investment Programs (PIP) Chapter 15: Ensuring Sound Macroeconomic PolicyPeter ParedesNo ratings yet
- Revised - Revised - Guidelines of SMAM - 4Document91 pagesRevised - Revised - Guidelines of SMAM - 4Clash Of Clans MasterNo ratings yet
- Complete Set GuidelinesDocument74 pagesComplete Set GuidelinesNavneet ValechaNo ratings yet
- Gih Project-Preparation Full-Document Final Art Web-2Document268 pagesGih Project-Preparation Full-Document Final Art Web-2Mohammed AbdullahNo ratings yet
- Ict 5Document130 pagesIct 5Gladys WambuiNo ratings yet
- Guideline of SMAM Scheme 20-21Document90 pagesGuideline of SMAM Scheme 20-21suraj jadhavNo ratings yet
- Technical Feasibility Report-uPVC Windows & DoorsDocument158 pagesTechnical Feasibility Report-uPVC Windows & Doorstechnopreneurvizag100% (1)
- GET FiT Performance Review and Baseline ReportDocument253 pagesGET FiT Performance Review and Baseline Reportocom706No ratings yet
- Diagnostic Study Report: DraftDocument74 pagesDiagnostic Study Report: DraftKumara PrasadNo ratings yet
- Investment ProgrammingDocument18 pagesInvestment ProgrammingSychelle Marie D. EscalanteNo ratings yet
- Chapter 14 Vigorously Advancing Science Technology and InnovationDocument13 pagesChapter 14 Vigorously Advancing Science Technology and InnovationPeter ParedesNo ratings yet
- SANRAL CombinedDocument284 pagesSANRAL CombinedPerentjana DjajaNo ratings yet
- PWC Budget Brief 2023Document61 pagesPWC Budget Brief 2023ttaashNo ratings yet
- CII-Benchmarking and Metrics PDFDocument11 pagesCII-Benchmarking and Metrics PDFAndrea DimayugaNo ratings yet
- Evoenergy-Attachment 5 Capital Expenditure-January 2018 - PublicDocument83 pagesEvoenergy-Attachment 5 Capital Expenditure-January 2018 - Publicshokobo123No ratings yet
- Final 0 Fiduciar 0 N 0 Program 000 P174650Document23 pagesFinal 0 Fiduciar 0 N 0 Program 000 P174650Rashedul IslamNo ratings yet
- APR FY14 (Complete)Document201 pagesAPR FY14 (Complete)Muhammad JamilNo ratings yet
- Corporate Strategic Plan Compressed 1Document123 pagesCorporate Strategic Plan Compressed 1Twino KartelNo ratings yet
- CITP Ebook CompleteDocument61 pagesCITP Ebook CompleteNurmahamira ZainiNo ratings yet
- ECBS Company Feasibility Study MainDocument70 pagesECBS Company Feasibility Study MainEmerging Capital Business SchoolNo ratings yet
- ZW&MA - Annual Report - FinalDocument76 pagesZW&MA - Annual Report - FinalTalo Contajazz Chileshe100% (2)
- LeanIX Poster 24 Key EA Views For Pharma ENDocument1 pageLeanIX Poster 24 Key EA Views For Pharma ENAB VenturesNo ratings yet
- GOB Project Approval Process: - A Scoping StudyDocument40 pagesGOB Project Approval Process: - A Scoping Studymithun dasNo ratings yet
- QHGDL 374 9Document53 pagesQHGDL 374 9Manal ZakiNo ratings yet
- Annual Report 2019-20Document170 pagesAnnual Report 2019-20ashish21sf1929No ratings yet
- #Finance and Procurement ManagementDocument14 pages#Finance and Procurement ManagementsougataNo ratings yet
- Session 1 - Introduction-LRAMSDocument23 pagesSession 1 - Introduction-LRAMSRANIL KLIM QUIRANTENo ratings yet
- AGENCY - APP - mPhilGEPS Training PresentationDocument24 pagesAGENCY - APP - mPhilGEPS Training PresentationRachel Abad-FabeNo ratings yet
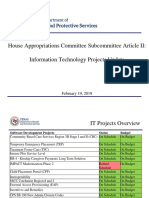
- House Appropriations Committee Subcommittee Article II: Information Technology Projects UpdateDocument10 pagesHouse Appropriations Committee Subcommittee Article II: Information Technology Projects UpdateSpit FireNo ratings yet
- Integrated LogisticsDocument48 pagesIntegrated LogisticsAkshay RaharNo ratings yet
- ISGPPHtmlPages - Documents - Docu - Reprt - POM Volume I Amended March 2021 - Final Vetted by WBDocument241 pagesISGPPHtmlPages - Documents - Docu - Reprt - POM Volume I Amended March 2021 - Final Vetted by WBAnuarul HoqueNo ratings yet
- Brick Klin MTR - Dec 7 2014 - 1Document115 pagesBrick Klin MTR - Dec 7 2014 - 1Mohiminul KhanNo ratings yet
- Infracompass 2020 Report Web OptimisedDocument273 pagesInfracompass 2020 Report Web OptimisedWondim TesfahunNo ratings yet
- RIDF Printed ManualeditedDocument81 pagesRIDF Printed ManualeditedTamilnadu Kaatumanarkovil100% (1)
- SIWP 2020 001 AML Fraud Detection Redhead FINAL MAY2021Document57 pagesSIWP 2020 001 AML Fraud Detection Redhead FINAL MAY2021Nour Allah tabibNo ratings yet
- Final UIIDP APA Guideline For 3rd APA.29.9.2020Document186 pagesFinal UIIDP APA Guideline For 3rd APA.29.9.2020Asmerom Mosineh100% (1)
- DTP CapDev Agenda BrgyDocument40 pagesDTP CapDev Agenda BrgyRoxanne Vicedo100% (1)
- Presentation To The Portfolio Committee On Finance: Information Can Change LivesDocument36 pagesPresentation To The Portfolio Committee On Finance: Information Can Change LivesThakur Avnish SinghNo ratings yet
- Gci 2017Document78 pagesGci 2017Halqa e YaranNo ratings yet
- DTP CapDev Agenda BrgyDocument40 pagesDTP CapDev Agenda BrgyBarangay MabuloNo ratings yet
- GovTech Maturity Index: The State of Public Sector Digital TransformationFrom EverandGovTech Maturity Index: The State of Public Sector Digital TransformationNo ratings yet
- A&N FactSheetDocument6 pagesA&N FactSheetShahid AliNo ratings yet
- +mahajan - Gupta Textbook of PSM, 4th Ed, 2013Document718 pages+mahajan - Gupta Textbook of PSM, 4th Ed, 2013Aparna Aby100% (2)
- 1435 PDFDocument23 pages1435 PDFShahid AliNo ratings yet
- PIP Process 2016-17 PDFDocument16 pagesPIP Process 2016-17 PDFShahid AliNo ratings yet
- Covid19 Vaccination Report Personnel LearnerDocument39 pagesCovid19 Vaccination Report Personnel LearnerAnalyn SamillanoNo ratings yet
- C2 ExamDocument29 pagesC2 ExamauNo ratings yet
- QuizDocument5 pagesQuizMARC JOSHUA SARANILLONo ratings yet
- AAH v2 Acute AsthmaDocument81 pagesAAH v2 Acute AsthmaEssa SmjNo ratings yet
- AHA ACLS Precourse Self Assessment Answers 2023Document32 pagesAHA ACLS Precourse Self Assessment Answers 2023R100% (4)
- Steps in Viral Pathogenesis-Lecture ThreeDocument3 pagesSteps in Viral Pathogenesis-Lecture ThreeIM CTNo ratings yet
- Murdhini TailaDocument11 pagesMurdhini TailaAaa BNo ratings yet
- NCP 5 Ovarian CancerDocument6 pagesNCP 5 Ovarian Cancersaint_ronald886% (29)
- The Effect of Kinesiotaping Therapy in Sciatic Patients in Pregnancy Due To Lumbar Disc Herniation According To Mckenzie's Extension Back ExerciseDocument3 pagesThe Effect of Kinesiotaping Therapy in Sciatic Patients in Pregnancy Due To Lumbar Disc Herniation According To Mckenzie's Extension Back ExerciseAna Lu LoboNo ratings yet
- ptj4008504 PDFDocument8 pagesptj4008504 PDFDiva VashtiNo ratings yet
- How To Remove Blackheads in Hindi: Jaane Asan TarekeDocument7 pagesHow To Remove Blackheads in Hindi: Jaane Asan TarekecshradhhaNo ratings yet
- Peripheral Nerve DisorderDocument23 pagesPeripheral Nerve DisorderSaman SarKoNo ratings yet
- Bleeding GumsDocument1 pageBleeding GumsalyssaNo ratings yet
- Do Vaccinations Cause Autism?Document3 pagesDo Vaccinations Cause Autism?Josh BarberaNo ratings yet
- Ministry of Health and Family Welfare Pregnancy GuidelinesDocument173 pagesMinistry of Health and Family Welfare Pregnancy GuidelinesKhushi GuptaNo ratings yet
- Study DesignDocument45 pagesStudy DesignDeepak SharmaNo ratings yet
- Types of Myocardial InfarctionDocument4 pagesTypes of Myocardial InfarctionntnquynhproNo ratings yet
- Money Tooth BookDocument41 pagesMoney Tooth BookVizi Adrian0% (2)
- TerjemahanDocument3 pagesTerjemahanRyski RahmaliaNo ratings yet
- Vaccination Is Child Abuse (Memes)Document62 pagesVaccination Is Child Abuse (Memes)guest100% (1)
- Case Study On PneumoniaDocument22 pagesCase Study On PneumoniaRuchika Kaushal100% (1)
- MRCP Paces DR Ahmed EliiwaDocument3 pagesMRCP Paces DR Ahmed EliiwaGhulamMemonNo ratings yet
- 01 The Limits of MedicalizationDocument12 pages01 The Limits of MedicalizationSaGa ZenJiNo ratings yet
- Anesthesiaforpituitary Surgery: Jinu Kim,, Ross Scott-MillerDocument10 pagesAnesthesiaforpituitary Surgery: Jinu Kim,, Ross Scott-MillerJose Miguel CastellonNo ratings yet
- 1106 FullDocument14 pages1106 Fullmarcos viniciusNo ratings yet
- Finding The Future of Care Provision The Role of Smart HospitalDocument10 pagesFinding The Future of Care Provision The Role of Smart HospitalDian Putri SusantiNo ratings yet
- Ac 72Document5 pagesAc 72Giovani TardiniNo ratings yet
- International Journal of Women's Dermatology: Mohsen Baghchechi, Jeffery Dunn, Navin Jaipaul, Sharon E. JacobDocument5 pagesInternational Journal of Women's Dermatology: Mohsen Baghchechi, Jeffery Dunn, Navin Jaipaul, Sharon E. JacobR JNo ratings yet
- Grade 10 - P.E and HealthDocument31 pagesGrade 10 - P.E and HealthLeah LamorinNo ratings yet
- Nephrology MCQ PDFDocument7 pagesNephrology MCQ PDFMonica J Ortiz PereiraNo ratings yet