You might also like
- Shoulder ExaminationDocument4 pagesShoulder ExaminationYS NateNo ratings yet
- Constant Score: Out-Patient Clinic Shoulder UnitDocument1 pageConstant Score: Out-Patient Clinic Shoulder Unitdeyaejar100% (1)
- Functional Test For Cervical SpineDocument1 pageFunctional Test For Cervical SpineJonathan Salvador GuinabayNo ratings yet
- CervicothoracicSpine AssessmentDocument16 pagesCervicothoracicSpine AssessmentKanika SinhaNo ratings yet
- Clinical Signs - NamedDocument9 pagesClinical Signs - NamedsprapurNo ratings yet
- MusculoskeletalDocument119 pagesMusculoskeletalEdissa PangilinanNo ratings yet
- Examination of Hand & Common Hand InjuriesDocument165 pagesExamination of Hand & Common Hand InjuriesPriya GK100% (1)
- Orthopaedic Emergencies: IC3 Musculoskeletal Teaching Week Gavin O'Reilly 6/1/15Document13 pagesOrthopaedic Emergencies: IC3 Musculoskeletal Teaching Week Gavin O'Reilly 6/1/15kylieverNo ratings yet
- Deformities of Greater and Lesser ToesDocument20 pagesDeformities of Greater and Lesser ToesSylvia ChongNo ratings yet
- Biomechanics of HipDocument27 pagesBiomechanics of Hipvj bharathNo ratings yet
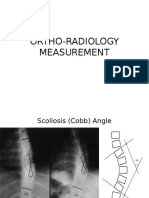
- Ortho Radiology MeasurementDocument25 pagesOrtho Radiology MeasurementNasrul Ha100% (1)
- Musculoskeletal TraumaDocument103 pagesMusculoskeletal TraumaJona Kristin EnclunaNo ratings yet
- Spinal Injury & Spinal Cord Injury: For General PracticeDocument60 pagesSpinal Injury & Spinal Cord Injury: For General PracticeRheselle LacuataNo ratings yet
- C SpineDocument33 pagesC SpineKarthickNo ratings yet
- HNP CervicalDocument33 pagesHNP CervicalIndra RanteNo ratings yet
- Diagnosis in Orthopaedic: David Hariadi Masjhoer SMF Orthopedi & Traumatologi RSUD A W SjahranieDocument24 pagesDiagnosis in Orthopaedic: David Hariadi Masjhoer SMF Orthopedi & Traumatologi RSUD A W SjahranieOkki Masitah Syahfitri NasutionNo ratings yet
- Computer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray ImagesDocument45 pagesComputer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray Imagesroky100% (1)
- Anterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationDocument31 pagesAnterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationNurul FajriNo ratings yet
- Queens Orthopedic Inpatient Trauma PDFDocument27 pagesQueens Orthopedic Inpatient Trauma PDFRema AmerNo ratings yet
- Biomechanics of The ElbowDocument16 pagesBiomechanics of The ElbowAsmaa Ahmad SharawyNo ratings yet
- Examination of The Knee Joint - RP's Ortho NotesDocument3 pagesExamination of The Knee Joint - RP's Ortho NotesSabari NathNo ratings yet
- Ankle Stability and MovementDocument40 pagesAnkle Stability and MovementBogdan GeangosNo ratings yet
- Basic Principles of Tendon TransferDocument10 pagesBasic Principles of Tendon TransferyeapdshengNo ratings yet
- Low BackDocument7 pagesLow BackMuhammad FahmyNo ratings yet
- Hand PDFDocument179 pagesHand PDFRadenSiwi Bagus HadhiningratNo ratings yet
- Dance Injuries-Foot and AnkleDocument7 pagesDance Injuries-Foot and Ankleapi-198787605100% (1)
- Kamars RadiologyDocument135 pagesKamars RadiologyNayantara Nair100% (1)
- Coxitis TB Hip KneeDocument26 pagesCoxitis TB Hip KneefajarvicNo ratings yet
- Splint and TractionsDocument40 pagesSplint and Tractionsakheel ahammed100% (1)
- Shoulderexaminationppt 180505152418Document19 pagesShoulderexaminationppt 180505152418KarthickNo ratings yet
- Low Back PainDocument8 pagesLow Back PainLev KalikaNo ratings yet
- Ankle FracturesDocument133 pagesAnkle FracturesAtiekPalludaNo ratings yet
- Trochanteric #Document20 pagesTrochanteric #Prakash AyyaduraiNo ratings yet
- Physeal Injuries FinalDocument49 pagesPhyseal Injuries FinalAnkit KarkiNo ratings yet
- Knee Biomechanics: Andrew CrosbyDocument32 pagesKnee Biomechanics: Andrew CrosbyBhanu Pratap PangteyNo ratings yet
- Clinical Anat Upper and Lower LimbDocument36 pagesClinical Anat Upper and Lower Limbtri_purnamasari_1No ratings yet
- Cavus FootDocument14 pagesCavus FootdrkbarryNo ratings yet
- Long Case OrthopaedicDocument24 pagesLong Case OrthopaedicSyimah UmarNo ratings yet
- Ankle Examination Orthopaedics McraeDocument6 pagesAnkle Examination Orthopaedics McraeHafizah HoshniNo ratings yet
- Acetabulam Approaches (Autosaved)Document57 pagesAcetabulam Approaches (Autosaved)Suniel MaheshwariNo ratings yet
- Achilles Tendon RuptureDocument6 pagesAchilles Tendon RuptureBn Wahyu AjiNo ratings yet
- B 756 Vertebris GB III10Document44 pagesB 756 Vertebris GB III10Lukasz Bartochowski100% (1)
- Physeal Injuries & Growth Disturbance: DR - GhaznaviDocument31 pagesPhyseal Injuries & Growth Disturbance: DR - GhaznavihaminatrafNo ratings yet
- Tuberculosis KneeDocument12 pagesTuberculosis KneePrasanna ChandiralingamNo ratings yet
- Special Tests For Elbow and ForearmDocument3 pagesSpecial Tests For Elbow and ForearmAllyza PenaNo ratings yet
- HIP JOINT Special Tests-WPS OfficeDocument51 pagesHIP JOINT Special Tests-WPS OfficeManisha MishraNo ratings yet
- Foot and Ankle ExamDocument6 pagesFoot and Ankle ExamTaizku_Kuzuryu_3630100% (1)
- Walking Gait-MUSCLES Involved PDFDocument2 pagesWalking Gait-MUSCLES Involved PDFlexi_2706No ratings yet
- Cervical Assessment Form 2014Document2 pagesCervical Assessment Form 2014Mark Koval100% (1)
- Toe and Foot ConditionsDocument14 pagesToe and Foot ConditionsNur InsyirahNo ratings yet
- FR Distal HumerusDocument55 pagesFR Distal Humerusiisscribd100% (1)
- Leg Ankle Orthopaedic Conditions FinalDocument26 pagesLeg Ankle Orthopaedic Conditions Finalangel bolfriNo ratings yet
- Ankle ExaminationDocument16 pagesAnkle Examinationbjpalmer100% (2)
- Tendon Injuries of Hand: DR Saumya AgarwalDocument101 pagesTendon Injuries of Hand: DR Saumya AgarwaltesfahuntekletilahunNo ratings yet
- Hip Joint 1Document22 pagesHip Joint 1foziiiii100% (2)
- Special Tests in Shoulder ExaminationDocument28 pagesSpecial Tests in Shoulder Examinationthwiseman100% (1)
- Biomechanics BHIP JOINTDocument68 pagesBiomechanics BHIP JOINTLinmayee SamalNo ratings yet
- Oh My Painful FOOT!!!: Plantar FasciitisDocument20 pagesOh My Painful FOOT!!!: Plantar FasciitisAsogaa MeteranNo ratings yet
- Bio Mechanics and Pathomechanics of Ankle JointDocument35 pagesBio Mechanics and Pathomechanics of Ankle Joint56 Vignesh j 079No ratings yet
- Bones and Joints TBDocument19 pagesBones and Joints TBmichaelcylNo ratings yet
- Open Fracture: BY, Kavinmithra VisuvanathenDocument57 pagesOpen Fracture: BY, Kavinmithra VisuvanathenzaimmuhtarNo ratings yet
- Dynamic Hip ScrewDocument6 pagesDynamic Hip ScrewzaimmuhtarNo ratings yet
- Partnering With Spousal Caregivers To Face The Challenges and The Heartbreak of Frontotemporal Dementia (FTD)Document54 pagesPartnering With Spousal Caregivers To Face The Challenges and The Heartbreak of Frontotemporal Dementia (FTD)zaimmuhtarNo ratings yet
- Central Diabetes Insipidus in Children and Young Adults: Etiological Diagnosis and Long-Term Outcome of Idiopathic CasesDocument9 pagesCentral Diabetes Insipidus in Children and Young Adults: Etiological Diagnosis and Long-Term Outcome of Idiopathic CaseszaimmuhtarNo ratings yet
- Central Diabetes Insipidus in Children and Young Adults: Etiological Diagnosis and Long-Term Outcome of Idiopathic CasesDocument9 pagesCentral Diabetes Insipidus in Children and Young Adults: Etiological Diagnosis and Long-Term Outcome of Idiopathic CaseszaimmuhtarNo ratings yet
- 02.08.13 Carpenter Case Presenation 1Document23 pages02.08.13 Carpenter Case Presenation 1zaimmuhtarNo ratings yet
- FF FK 46-15 Per P - AdlnDocument8 pagesFF FK 46-15 Per P - AdlnzaimmuhtarNo ratings yet
- Peripartum Cardiomyopathy: Current Management and Future PerspectivesDocument8 pagesPeripartum Cardiomyopathy: Current Management and Future PerspectiveszaimmuhtarNo ratings yet
- Seminars in Diagnostic Pathology Volume 30 Issue 1 2013 (Doi 10.1053 - J.semdp.2012.01.003) Requena, Luis Kutzner, Heinz - HemangioendotheliomaDocument16 pagesSeminars in Diagnostic Pathology Volume 30 Issue 1 2013 (Doi 10.1053 - J.semdp.2012.01.003) Requena, Luis Kutzner, Heinz - HemangioendotheliomazaimmuhtarNo ratings yet
- Journal of Clinical Anesthesia: Original ContributionDocument6 pagesJournal of Clinical Anesthesia: Original ContributionzaimmuhtarNo ratings yet
- JeradDocument10 pagesJeradzaimmuhtarNo ratings yet
- Travel MedicineDocument40 pagesTravel MedicinezaimmuhtarNo ratings yet
- Teaching Slide Set 2019: Global Initiative For Chronic Obstructive Lung Disease (Gold)Document135 pagesTeaching Slide Set 2019: Global Initiative For Chronic Obstructive Lung Disease (Gold)zaimmuhtar100% (1)
- Nellhaus ChartDocument1 pageNellhaus ChartZsa Zsa Maranani100% (2)
- Judicial Hanging Cause of DeathDocument3 pagesJudicial Hanging Cause of Deathzaimmuhtar100% (1)
- Shoulder DislocationDocument13 pagesShoulder DislocationSahoo PRASANTANo ratings yet
- NUR 602 Musculoskeletal System Student HandoutDocument35 pagesNUR 602 Musculoskeletal System Student HandoutChristine Joy MolinaNo ratings yet
- Skeletal System PowerPointDocument37 pagesSkeletal System PowerPointScience,Physical Education And Sports Videos100% (1)
- Lower Limb Orthosis: Dr. Sumit Raghav, PT Assistant Professor Jyotirao Subharti College of PhysiotherapyDocument56 pagesLower Limb Orthosis: Dr. Sumit Raghav, PT Assistant Professor Jyotirao Subharti College of PhysiotherapyKavya Mittal100% (2)
- Blandino We0413Document25 pagesBlandino We0413RohitOkeNo ratings yet
- Esquina Posteromedial RodillaDocument9 pagesEsquina Posteromedial RodillaSebastian RamirezNo ratings yet
- Dance Injuries Power PointDocument20 pagesDance Injuries Power PointJerry Capitulo PorlucasNo ratings yet
- 10 Best For RowingDocument15 pages10 Best For RowingVictor Laurent BigotNo ratings yet
- Providing ROM ExercisesDocument3 pagesProviding ROM ExercisesjhommmmmNo ratings yet
- 155 Jason KarpDocument4 pages155 Jason KarpNeuNo ratings yet
- Front Squat - CrossFit Training GuideDocument2 pagesFront Squat - CrossFit Training GuideKarim HaridiNo ratings yet
- Semester 2 - Module 4 (Musculo-Skeletal System)Document10 pagesSemester 2 - Module 4 (Musculo-Skeletal System)Hazmi Al-WafiNo ratings yet
- Dynamic Warm-Up ExercisesDocument6 pagesDynamic Warm-Up ExercisesOtaku ChanNo ratings yet
- HIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10Document116 pagesHIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10joe joeNo ratings yet
- Arm Diagram Left - Google Search PDFDocument1 pageArm Diagram Left - Google Search PDFjordanNo ratings yet
- Shinryukan Stretching ProgramDocument28 pagesShinryukan Stretching Programwilera100% (1)
- Muscle BiomechanicsDocument40 pagesMuscle BiomechanicsDr. Deepshikha ThakurNo ratings yet
- IndianJPhysTherRes1279-7599768 210637Document10 pagesIndianJPhysTherRes1279-7599768 210637mNo ratings yet
- Strength and Conditioning For Fencing.13Document6 pagesStrength and Conditioning For Fencing.13gregory tzortziadis100% (1)
- Miracle 7Document9 pagesMiracle 7Harry Sivia100% (2)
- Ue RomDocument5 pagesUe Romnacole78No ratings yet
- KneeDocument8 pagesKneeAnonymous Aud8lt9No ratings yet
- ICD-9-CM Codes: ICF Codes:: d4452 Reaching (Using The Hands and Arms To ExtendDocument13 pagesICD-9-CM Codes: ICF Codes:: d4452 Reaching (Using The Hands and Arms To ExtendAbdul Wahid ShaikhNo ratings yet
- Joints Movements in Planes and AxesDocument1 pageJoints Movements in Planes and AxesNaveera GhouriNo ratings yet
- B.E - I Yr 2018-19 FR ClassesDocument220 pagesB.E - I Yr 2018-19 FR ClassesMatam PrasadNo ratings yet
- Accessory LigamentsDocument10 pagesAccessory LigamentsWidy AnniNo ratings yet
- The Importance of Gluteus Medius in The CyclistDocument3 pagesThe Importance of Gluteus Medius in The CyclistFrancisco Javier HerreraNo ratings yet
- MapehasdasdDocument2 pagesMapehasdasdAmiel Angelo BaliosNo ratings yet
- Case Presentation: Anterior Cruciate Ligament (ACL) Rupture Oscar NG 09037032DDocument23 pagesCase Presentation: Anterior Cruciate Ligament (ACL) Rupture Oscar NG 09037032DOscar NgNo ratings yet