You might also like
- Stretch Guide'Document57 pagesStretch Guide'samyak jainNo ratings yet
- Atlas Human Anatomy Ciba NetterDocument641 pagesAtlas Human Anatomy Ciba Netterxxxx79% (28)
- Sexually Transmitted Disease (STD)Document102 pagesSexually Transmitted Disease (STD)uhurtme100% (10)
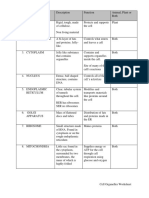
- Cell Organelles WorksheetDocument8 pagesCell Organelles WorksheetJohn OsborneNo ratings yet
- Leishmaniasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLeishmaniasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Swedish Massage InfoDocument5 pagesSwedish Massage InfoJoy CelestialNo ratings yet
- Dermatofitosis FitzpatrickDocument28 pagesDermatofitosis FitzpatrickFadli IlhamNo ratings yet
- Tables VirusesDocument9 pagesTables VirusesOmphile DansonNo ratings yet
- LeishmaniasisDocument32 pagesLeishmaniasisPeachy PieNo ratings yet
- Human Anatomy and Physiology NotesDocument33 pagesHuman Anatomy and Physiology NotesFLORLYN VERALNo ratings yet
- Chapter 8 The Endocrine SystemDocument56 pagesChapter 8 The Endocrine SystemSainuddinSaddinNo ratings yet
- LeishmaniasisDocument77 pagesLeishmaniasisjaveria choudharyNo ratings yet
- MCQ FMS 4 (2016) With AnswersDocument13 pagesMCQ FMS 4 (2016) With Answersstella pangestikaNo ratings yet
- Human Body Systems Lesson Plan 3Document3 pagesHuman Body Systems Lesson Plan 3api-338430889100% (1)
- Leishmaniasis PresentationDocument65 pagesLeishmaniasis PresentationAli ChaudhryNo ratings yet
- CandidiasisDocument27 pagesCandidiasisfarmasi_hmNo ratings yet
- Krizia Joy Borromeo-Galve, MD: Bulacan Medical Center, Department of PediatricsDocument84 pagesKrizia Joy Borromeo-Galve, MD: Bulacan Medical Center, Department of PediatricsTara Oliveros Dela CruzNo ratings yet
- Leishmaniasis LecturioDocument12 pagesLeishmaniasis LecturioPranjali WeladiNo ratings yet
- LeishmaniaDocument59 pagesLeishmaniaEINSTEIN2DNo ratings yet
- 2-15 MycobacteSdASDASDASDAria NOTESDocument14 pages2-15 MycobacteSdASDASDASDAria NOTESbassist1089No ratings yet
- Blood & Tissue Protozoa-II: Prof - Dr.Shaheen Sharafat MBBS.M.Phil PH.D Dept - of Pathology LNH&MCDocument47 pagesBlood & Tissue Protozoa-II: Prof - Dr.Shaheen Sharafat MBBS.M.Phil PH.D Dept - of Pathology LNH&MCHumna JawedNo ratings yet
- Git 1 PDFDocument24 pagesGit 1 PDFafaq alismailiNo ratings yet
- Leishmaniasis 2438Document36 pagesLeishmaniasis 2438Caroline NanditaNo ratings yet
- Zoonotic VirusesDocument12 pagesZoonotic VirusesSamuel Ojonugwa AuduNo ratings yet
- Diagnosis of Leishmaniasis: Review ArticleDocument12 pagesDiagnosis of Leishmaniasis: Review ArticleTUfoodbiotech groupNo ratings yet
- Leishmania SisDocument37 pagesLeishmania Sis1x CzNo ratings yet
- Arenavirus ReportDocument18 pagesArenavirus ReportAce Ashley BaronNo ratings yet
- Bacte Grams Neg CocciDocument10 pagesBacte Grams Neg CocciErika PatarayNo ratings yet
- 2017 Cutaneous T Cell Lymphoma (CTCL) Superimposed On Disseminated Cutaneous Leishmaniasis (DCL) in An Immunocompromised Female From YemenDocument5 pages2017 Cutaneous T Cell Lymphoma (CTCL) Superimposed On Disseminated Cutaneous Leishmaniasis (DCL) in An Immunocompromised Female From YemenuisjesusajNo ratings yet
- History Taking in DermatologyDocument18 pagesHistory Taking in DermatologyAisha MohamedNo ratings yet
- Leishmaniasis. Neglected DiseaseDocument10 pagesLeishmaniasis. Neglected DiseaseEli FloresNo ratings yet
- 1) Cutaneous LeishmaniasisDocument3 pages1) Cutaneous LeishmaniasisDjdjjd SiisusNo ratings yet
- 016 LeishmaniasisDocument6 pages016 LeishmaniasisSkshah1974No ratings yet
- 1) Cutaneous LeishmaniasisDocument3 pages1) Cutaneous LeishmaniasisIM CTNo ratings yet
- Acid Fast Bacteria: M. Tuberculosis, M. LepraeDocument22 pagesAcid Fast Bacteria: M. Tuberculosis, M. LepraeelaNo ratings yet
- Jordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDocument19 pagesJordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDaniel AtiehNo ratings yet
- Mr. K. Sesha Kumar, M.SC (N) ,: Nursing Tutor, ESIC College of Nursing, Indira Nagar, BangaloreDocument37 pagesMr. K. Sesha Kumar, M.SC (N) ,: Nursing Tutor, ESIC College of Nursing, Indira Nagar, BangaloreK Sesha KumarNo ratings yet
- Nelson A. Salazar, M.SC., DLSHTM, PH.DDocument129 pagesNelson A. Salazar, M.SC., DLSHTM, PH.DAlejandra CañasNo ratings yet
- LeprosyDocument110 pagesLeprosyNguyễn ThànhNo ratings yet
- FilariaDocument16 pagesFilariaJessa MayNo ratings yet
- Oral Pathology ChaptersDocument8 pagesOral Pathology ChaptersHazem MouradNo ratings yet
- Virus (Ania KPD, DR., MKes)Document55 pagesVirus (Ania KPD, DR., MKes)Gita RizkiNo ratings yet
- HERPESVIRUSES, PARVO 2021 Students - KopieDocument38 pagesHERPESVIRUSES, PARVO 2021 Students - KopieMr.FantasthiccNo ratings yet
- Cutaneous Leishmaniasis: Mark S. Bailey, MRCP, Diana N.J. Lockwood, BSC, MD, FRCPDocument9 pagesCutaneous Leishmaniasis: Mark S. Bailey, MRCP, Diana N.J. Lockwood, BSC, MD, FRCPeva yustianaNo ratings yet
- Microbiology PinkDocument3 pagesMicrobiology PinkBenjamin GaliaNo ratings yet
- 150 - Mycobacterium LepraeDocument83 pages150 - Mycobacterium LepraeNirav PatelNo ratings yet
- Leishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal MedicineDocument20 pagesLeishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal MedicineSHIHAB UDDIN KAZINo ratings yet
- Lecture 52 - 3rd Asessment - Lei SH ManiaDocument45 pagesLecture 52 - 3rd Asessment - Lei SH Maniaapi-3703352No ratings yet
- Leishmaniasis KuliahDocument28 pagesLeishmaniasis KuliahNadiya KusnadiNo ratings yet
- Viral InfectionsDocument23 pagesViral InfectionsMiguel Cuevas DolotNo ratings yet
- HPV and Other VirusesDocument47 pagesHPV and Other VirusesWai Kwong ChiuNo ratings yet
- Mycobacterium LepraeDocument3 pagesMycobacterium Lepraeanupama menonNo ratings yet
- Jordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDocument19 pagesJordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDaniel AtiehNo ratings yet
- Bacterial Meningitis CaseDocument24 pagesBacterial Meningitis CaseALI MUMTAZNo ratings yet
- Case Study of Black Death: Our Lady of Fatima UniversityDocument7 pagesCase Study of Black Death: Our Lady of Fatima UniversityJanna PimentelNo ratings yet
- ArenavirusDocument29 pagesArenavirusRamirez GiovarNo ratings yet
- Kala AzarDocument25 pagesKala AzarVanitha ReddyNo ratings yet
- Revew Leish Citocinas 2000Document4 pagesRevew Leish Citocinas 2000Helen AguiarNo ratings yet
- Insignis Pedia MMRV LopezDocument7 pagesInsignis Pedia MMRV LopezChrisfernan MondragonNo ratings yet
- Blood and Tissue FlagellatesDocument27 pagesBlood and Tissue FlagellatesAtef HusseinNo ratings yet
- Gineco - Eu ArticolDocument4 pagesGineco - Eu ArticolFlorentina-Alexandra DobrescuNo ratings yet
- 744 Mycobacterium LepraeDocument83 pages744 Mycobacterium Lepraeabhiaishu.kanna26No ratings yet
- The Great Imitator A Rare Case of Lues Maligna in An Hiv Positive Patient 4Document4 pagesThe Great Imitator A Rare Case of Lues Maligna in An Hiv Positive Patient 4Talaat OmranNo ratings yet
- Therapy of Cutaneous Leishmaniasis: ReviewDocument8 pagesTherapy of Cutaneous Leishmaniasis: ReviewEm liNo ratings yet
- Netter's Internal Medicine 2nd Ed 19Document10 pagesNetter's Internal Medicine 2nd Ed 19Panagiotis SouldatosNo ratings yet
- Kvir 13 2074130Document33 pagesKvir 13 2074130Robert StryjakNo ratings yet
- 2 Oral UlcersDocument27 pages2 Oral UlcersAhmed Abdelhady Mahmoud AbdelwahedNo ratings yet
- BSC (Medical Lab Technology) 28.02.2018Document38 pagesBSC (Medical Lab Technology) 28.02.2018Vamsi ReddyNo ratings yet
- Pharyngitis SiccaDocument3 pagesPharyngitis SiccaEdris SharifiNo ratings yet
- Matary Surgical Anatomy 2013 AllTebFamily ComDocument320 pagesMatary Surgical Anatomy 2013 AllTebFamily Comrusu_alexandra_4No ratings yet
- Gingival Absorption of Rat Periodontal Disease Model and Rat Tooth Movement ModelDocument7 pagesGingival Absorption of Rat Periodontal Disease Model and Rat Tooth Movement ModelLouis HutahaeanNo ratings yet
- Hematopoiesis: Pluri - Several) or Hemocytoblasts. These Cells Have The Capacity To Develop Into Many Different Types ofDocument12 pagesHematopoiesis: Pluri - Several) or Hemocytoblasts. These Cells Have The Capacity To Develop Into Many Different Types ofRajender ArutlaNo ratings yet
- Bio270 Tutorial Week 10Document2 pagesBio270 Tutorial Week 10Mirza KarmilaNo ratings yet
- Blood ClottingDocument3 pagesBlood Clottingridwan100% (9)
- Anatomy LandmarkDocument31 pagesAnatomy LandmarkWildan Humairah33% (3)
- Immunochemistry and BiosensorsDocument13 pagesImmunochemistry and BiosensorsPalak AgarwalNo ratings yet
- 2 NDLPDocument14 pages2 NDLPJennifer Lopez Guiao-Catacutan0% (1)
- Medical Terminolog1Document25 pagesMedical Terminolog1Jullia SollezaNo ratings yet
- ArchegoniateplantDocument21 pagesArchegoniateplantShubhamMalikNo ratings yet
- PHEOCHROMOCYTOMADocument28 pagesPHEOCHROMOCYTOMAQueenElsaNo ratings yet
- Grade 6 DLP Q2 W1D1Document14 pagesGrade 6 DLP Q2 W1D1CRISTINE ANN ARANDIANo ratings yet
- Lab 1 - Plant Cells and TissuesDocument8 pagesLab 1 - Plant Cells and TissuesArushiSoodNo ratings yet
- Model Answers: Chapter 13 Homeostasis and The Human Urinary SystemDocument3 pagesModel Answers: Chapter 13 Homeostasis and The Human Urinary Systemsyed aliNo ratings yet
- Pex 03 09Document5 pagesPex 03 09Kinea1100% (3)
- Circulatory System of CockroachDocument18 pagesCirculatory System of Cockroachyayeg rajaNo ratings yet
- Endometriosis & AdenomyosisDocument54 pagesEndometriosis & AdenomyosisKapil StaleyNo ratings yet
- Patologi Sistem Pencernaan Hati Sesi 1aDocument36 pagesPatologi Sistem Pencernaan Hati Sesi 1adewinurfadilahNo ratings yet
- Torso GuideDocument373 pagesTorso GuideMonica PatracutaNo ratings yet
- Laboratory Evaluation of HemostasisDocument7 pagesLaboratory Evaluation of HemostasisGerly MaglangitNo ratings yet