You might also like
- Invasive Pulmonary Aspergi Llosis: Seminars in Respiratory and Critical Care MedicineDocument24 pagesInvasive Pulmonary Aspergi Llosis: Seminars in Respiratory and Critical Care MedicineChengShiun ShiueNo ratings yet
- Anti GBM DiseaseDocument36 pagesAnti GBM DiseaseHemanth PrakashNo ratings yet
- Emergency Diabetes 2023 - Septian Mixrova SebayangDocument30 pagesEmergency Diabetes 2023 - Septian Mixrova SebayangFiqri DzulfaqqorNo ratings yet
- สำเนา draft1 - DKA 1Document42 pagesสำเนา draft1 - DKA 1teddypor100% (1)
- Evans2021 Article SurvivingSepsisCampaignInternaDocument67 pagesEvans2021 Article SurvivingSepsisCampaignInternaPablo Antonio Cruz VivasNo ratings yet
- Expanding Consensus in Portal HypertensionDocument29 pagesExpanding Consensus in Portal HypertensionJosé Pepo Apey Reinoso100% (1)
- Cerebro Perdedor de SalDocument14 pagesCerebro Perdedor de SalGabyRamónNo ratings yet
- Non Rheumatic CarditisDocument13 pagesNon Rheumatic CarditisJavier SaadNo ratings yet
- Surviving Sepsis Campaign 2021 Guidelines Infographic Vasoactive AgentDocument1 pageSurviving Sepsis Campaign 2021 Guidelines Infographic Vasoactive AgentAnsel AriaNo ratings yet
- Shunts, Memorix & Oxygenation ParametersDocument54 pagesShunts, Memorix & Oxygenation ParametersVero DuranNo ratings yet
- Deep Venous ThrombosisDocument28 pagesDeep Venous ThrombosisJavier CubillosNo ratings yet
- Hyperglycemia in Acute StrokeDocument4 pagesHyperglycemia in Acute StrokeDewi PratiwiNo ratings yet
- Enfermedad Renal CronicaDocument11 pagesEnfermedad Renal CronicafranciscoNo ratings yet
- Neutropenic Fever: Dr. Meral SönmezoğluDocument67 pagesNeutropenic Fever: Dr. Meral SönmezoğluOguzcan KinikogluNo ratings yet
- Lesion Renal AgudaDocument28 pagesLesion Renal AgudaCarlitos Antonio100% (1)
- Coherencia HemodinamicaDocument9 pagesCoherencia HemodinamicaMaritza Alejandra Baeza EricesNo ratings yet
- Acute On Chronic Liver Failure: Ulva Yogia GuslafDocument19 pagesAcute On Chronic Liver Failure: Ulva Yogia GuslafSyahrul AdzimNo ratings yet
- Encefalopatia HepaticaDocument4 pagesEncefalopatia HepaticaMaria Alexandra BanutaNo ratings yet
- Understanding Bronchiectasis: Causes, Symptoms and TreatmentDocument60 pagesUnderstanding Bronchiectasis: Causes, Symptoms and TreatmentArulNo ratings yet
- Guia 13481Document22 pagesGuia 13481CarmenNo ratings yet
- Tep Nejm 2022Document13 pagesTep Nejm 2022Jorge CastilloNo ratings yet
- Chronic Leukemia DR Moses KazevuDocument46 pagesChronic Leukemia DR Moses KazevuMoses Jr KazevuNo ratings yet
- 04 ShockDocument142 pages04 ShockDefa3 madniNo ratings yet
- EmpiemaDocument19 pagesEmpiemaArrol Iswahyudi100% (1)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- CKD Stages and ManagementDocument23 pagesCKD Stages and ManagementArvindan Subramaniam100% (1)
- Spektrum AIDocument55 pagesSpektrum AIOgizWaraNo ratings yet
- Lecture 6 Sickle Cell AnaemiaDocument33 pagesLecture 6 Sickle Cell AnaemiaKingsley AdebayoNo ratings yet
- 5 Tuberculosis GenitalDocument6 pages5 Tuberculosis GenitalBrian Jhesit GarciaNo ratings yet
- CardioplegiaDocument1 pageCardioplegiaapi-541766630No ratings yet
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeJawad SaleemNo ratings yet
- Acute Kidney InjuryDocument60 pagesAcute Kidney InjuryAbegail Fermanejo-GeneraoNo ratings yet
- Fitz Hugh Curtis SyndromeDocument7 pagesFitz Hugh Curtis SyndromecomunianNo ratings yet
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaNo ratings yet
- Shock Hemorrágico PDFDocument10 pagesShock Hemorrágico PDFMillerAponteNo ratings yet
- PneumoniaDocument120 pagesPneumoniaSaklenali LoniNo ratings yet
- MULTIPLE MYELOMA For Medical Students. Copy - 032148Document39 pagesMULTIPLE MYELOMA For Medical Students. Copy - 032148Miracle Odenigbo100% (1)
- Glomerular Diseases and Pathogenesis of Kidney InflammationDocument22 pagesGlomerular Diseases and Pathogenesis of Kidney InflammationrizapuspairyaniNo ratings yet
- Infectious Diseases (1&2) : TuberculosisDocument67 pagesInfectious Diseases (1&2) : TuberculosisYesi SaputriNo ratings yet
- Chronic Kidney DiseaseDocument40 pagesChronic Kidney DiseasePaul SinsNo ratings yet
- Adrenal DisordersDocument32 pagesAdrenal DisordersJyoti ChadhaNo ratings yet
- Classification and Causes of Anemia ExplainedDocument30 pagesClassification and Causes of Anemia ExplainedhercolaniumNo ratings yet
- Dual Antiplatelet Therapy Vs Alteplase For Patients With Minor NondisablingDocument10 pagesDual Antiplatelet Therapy Vs Alteplase For Patients With Minor Nondisablingbetongo Bultus Ocultus XVNo ratings yet
- Pneumonia 1Document53 pagesPneumonia 1Sardor AnorboevNo ratings yet
- Diabetes MellitusDocument42 pagesDiabetes Mellitusalexandra chimboNo ratings yet
- Lecture 10 - Hemolytic Anemias - Extracorpuscular DefectsDocument28 pagesLecture 10 - Hemolytic Anemias - Extracorpuscular DefectsArif MaulanaNo ratings yet
- SepsisDocument33 pagesSepsisv_vijayakanth7656No ratings yet
- Chronic Kidney Disease Stages, Risk Factors, and TreatmentDocument45 pagesChronic Kidney Disease Stages, Risk Factors, and Treatmentnaro ayosNo ratings yet
- Neurological Manifestations of HIV/AIDSDocument34 pagesNeurological Manifestations of HIV/AIDSashuNo ratings yet
- Chronic Hypertension in Pregnancy: Clinical PracticeDocument8 pagesChronic Hypertension in Pregnancy: Clinical PracticeemmoyNo ratings yet
- FBC Interpretation and Function of Blood ComponentsDocument7 pagesFBC Interpretation and Function of Blood ComponentsFrancesca LiNo ratings yet
- Alport Syndrome Genetic ResearchDocument4 pagesAlport Syndrome Genetic ResearchVenson CeaNo ratings yet
- ESICM Guidelines On ARDS 2023Document33 pagesESICM Guidelines On ARDS 2023ctsakalakisNo ratings yet
- Pneumocystis Carinii PneumoniaDocument16 pagesPneumocystis Carinii PneumoniaHera HeraNo ratings yet
- IDSA - Guía de Infección Asociada A Catéter VenosoDocument45 pagesIDSA - Guía de Infección Asociada A Catéter Venosoivonne micoltaNo ratings yet
- Distinguishing TRALI and TACODocument6 pagesDistinguishing TRALI and TACOl1o2stNo ratings yet
- Managing Febrile Neutropenia in Pediatric Oncology PatientsDocument38 pagesManaging Febrile Neutropenia in Pediatric Oncology Patientsdr FAHADKHALIQSIALNo ratings yet
- Interstit NephDocument18 pagesInterstit NephpashaNo ratings yet
- IvabradineDocument30 pagesIvabradinepashaNo ratings yet
- Interstit NephDocument18 pagesInterstit NephpashaNo ratings yet
- IvabradineDocument33 pagesIvabradinepashaNo ratings yet
- IvabradineDocument2 pagesIvabradinepashaNo ratings yet
- IvabradineDocument30 pagesIvabradinepashaNo ratings yet
- Geriatric MCQsDocument3 pagesGeriatric MCQspasha100% (2)
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDocument2 pagesThis Is An Electronic Report & Not: To Be Used For Any Legal PurposespashaNo ratings yet
- Geriatric MCQsDocument3 pagesGeriatric MCQspasha100% (2)
- Alternative NamesDocument67 pagesAlternative NamespashaNo ratings yet
- Wa0167Document1 pageWa0167pashaNo ratings yet
- Chronic Kidney Disease: Causes, Symptoms, Diagnosis and TreatmentDocument67 pagesChronic Kidney Disease: Causes, Symptoms, Diagnosis and TreatmentpashaNo ratings yet
- Wild WadiDocument1 pageWild WadipashaNo ratings yet
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDocument2 pagesThis Is An Electronic Report & Not: To Be Used For Any Legal PurposespashaNo ratings yet
- Wild WadiDocument1 pageWild WadipashaNo ratings yet
- Everyday Challenges in Clinical Practice: Peshawar Meeting November 2017Document41 pagesEveryday Challenges in Clinical Practice: Peshawar Meeting November 2017pashaNo ratings yet
- Regestration FormDocument1 pageRegestration FormAnonymous XcSBqeNo ratings yet
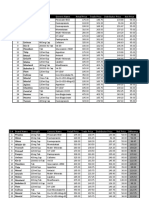
- Drug price comparison tableDocument2 pagesDrug price comparison tablepashaNo ratings yet
- FFFFFFFDocument72 pagesFFFFFFFpashaNo ratings yet
- PSH 2017 Meeting Highlights Risk Assessment Liver Disease SurgeryDocument77 pagesPSH 2017 Meeting Highlights Risk Assessment Liver Disease SurgerypashaNo ratings yet
- JKHFDSJFHKDocument23 pagesJKHFDSJFHKpashaNo ratings yet
- National Guideline On TBDocument82 pagesNational Guideline On TBpashaNo ratings yet
- PSH 2017 Meeting Highlights Risk Assessment Liver Disease SurgeryDocument77 pagesPSH 2017 Meeting Highlights Risk Assessment Liver Disease SurgerypashaNo ratings yet
- PSH 2017 Meeting Highlights Risk Assessment Liver Disease SurgeryDocument77 pagesPSH 2017 Meeting Highlights Risk Assessment Liver Disease SurgerypashaNo ratings yet
- Cardiogenic ShockDocument42 pagesCardiogenic ShockpashaNo ratings yet
- National Guideline On TBDocument82 pagesNational Guideline On TBpashaNo ratings yet
- PSH 2017 Meeting Highlights Risk Assessment Liver Disease SurgeryDocument77 pagesPSH 2017 Meeting Highlights Risk Assessment Liver Disease SurgerypashaNo ratings yet
- Aortic Dissection: DR Muhammad Burhan PashaDocument41 pagesAortic Dissection: DR Muhammad Burhan PashapashaNo ratings yet
- CKD Anaemia Guide: Causes, Symptoms, TreatmentDocument35 pagesCKD Anaemia Guide: Causes, Symptoms, TreatmentpashaNo ratings yet
- Cell Bio Final SOS PackageDocument51 pagesCell Bio Final SOS PackageMegadirectioner 21No ratings yet
- Microbiology Question Paper 1st TermDocument2 pagesMicrobiology Question Paper 1st TermSourav GhoshNo ratings yet
- Introduction To HaemostasisDocument18 pagesIntroduction To Haemostasiswatchme3No ratings yet
- Singh 2018Document16 pagesSingh 2018Georgiana BunghiuzNo ratings yet
- Pembahasan Seminar Part 2 Agustus 2017Document971 pagesPembahasan Seminar Part 2 Agustus 2017Kemal Fikar MuhammadNo ratings yet
- Antiviral Medicines and Vaccines Sum PDFDocument118 pagesAntiviral Medicines and Vaccines Sum PDFIntuch SikareepaisanNo ratings yet
- Agriculture Mcqs PDFDocument4 pagesAgriculture Mcqs PDFsarfraz2688No ratings yet
- GEN. BIOLOGY 1: CELL CYCLE AND MEIOSISDocument5 pagesGEN. BIOLOGY 1: CELL CYCLE AND MEIOSISAna Carmela MortelNo ratings yet
- Ref 4Document13 pagesRef 4indah setiyaniNo ratings yet
- Chemotherapeutic Agents in Periodontal DiseasesDocument8 pagesChemotherapeutic Agents in Periodontal Diseasesapi-3861216No ratings yet
- Allergy: DR Panini Patankar Guide: DR Shirish JoshiDocument53 pagesAllergy: DR Panini Patankar Guide: DR Shirish JoshiPanini PatankarNo ratings yet
- 35 Facts and Reasons Why I Became An Avid Ex-Vaxxer and No Longer Vaccinate PDFDocument39 pages35 Facts and Reasons Why I Became An Avid Ex-Vaxxer and No Longer Vaccinate PDFmvrosuNo ratings yet
- Cell Organelles and Their Government Department ComparisonsDocument5 pagesCell Organelles and Their Government Department ComparisonsJenica CruzNo ratings yet
- FungiDocument4 pagesFungiMayda RiveraNo ratings yet
- PCAP-c Group A NiggasDocument39 pagesPCAP-c Group A NiggasJenny YenNo ratings yet
- Glossary of Endodontic Terms - UPDATED MARCH 2020 050720 PDFDocument48 pagesGlossary of Endodontic Terms - UPDATED MARCH 2020 050720 PDFBenjiNo ratings yet
- Reading ComprehensionDocument15 pagesReading Comprehensionemi agus triani100% (2)
- I PREVENT COVID FLU RSV Clinical GuideDocument15 pagesI PREVENT COVID FLU RSV Clinical GuideServaas OostrikNo ratings yet
- 1607613832Document646 pages1607613832Andrei-Dorin BicaNo ratings yet
- Cell CommunicationDocument32 pagesCell CommunicationMajd MerieNo ratings yet
- Class 9 Biology Chapter 16 Diseases Causes and ControlDocument6 pagesClass 9 Biology Chapter 16 Diseases Causes and ControlwanroyNo ratings yet
- Genetics Problems WorksheetDocument5 pagesGenetics Problems WorksheettaylorNo ratings yet
- COVID-19 Affect On SportsDocument6 pagesCOVID-19 Affect On SportsMalik AhzanNo ratings yet
- Gbbe Chapter 2 CancerDocument20 pagesGbbe Chapter 2 Cancerapi-374854456No ratings yet
- Cytokines 1 PDFDocument1 pageCytokines 1 PDFzalmezeydNo ratings yet
- Chemical Carcinogenesis I and Ii: Michael Lea 2016Document31 pagesChemical Carcinogenesis I and Ii: Michael Lea 2016aasiyaNo ratings yet
- Renal EmergenciesDocument93 pagesRenal EmergenciesShubham gaurNo ratings yet
- Preparedness For A High-Impact Respiratory Pathogen Pandemic PDFDocument84 pagesPreparedness For A High-Impact Respiratory Pathogen Pandemic PDFchinzsteelNo ratings yet
- Nelsons-Cytogenetics ChapterDocument26 pagesNelsons-Cytogenetics ChapterMicah Lou CalambaNo ratings yet
- Joy Benemor - Infection and response exam QsDocument8 pagesJoy Benemor - Infection and response exam Qsv2jj5qfhjpNo ratings yet