You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- List of Medicines and Corresponding Maximum Drug Retail PriceDocument3 pagesList of Medicines and Corresponding Maximum Drug Retail PriceLindbergh Espino100% (4)
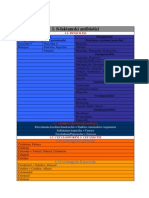
- Classification of AntibioticsDocument5 pagesClassification of AntibioticsdenaNo ratings yet
- Pediatric Antibiotic Dosing ChartDocument1 pagePediatric Antibiotic Dosing Chartjimy babiNo ratings yet
- Nafdac Approved Pesticides in NigeriaDocument56 pagesNafdac Approved Pesticides in NigeriaAnonymous xZfbfF7SQJ73% (22)
- Suppliers MasterfileDocument150 pagesSuppliers Masterfilejayesmine barlongay100% (1)
- Lina Agustina 10117087 B Ing Tugas II PDFDocument15 pagesLina Agustina 10117087 B Ing Tugas II PDFLina AgustinaNo ratings yet
- Lina Agustina 10117087 B Inggris Tugas PDFDocument8 pagesLina Agustina 10117087 B Inggris Tugas PDFLina AgustinaNo ratings yet
- Lina Agustina 10117087 B Inggris Tugas PDFDocument8 pagesLina Agustina 10117087 B Inggris Tugas PDFLina AgustinaNo ratings yet
- Lina Agustina 10117087 B Ing Tugas II PDFDocument15 pagesLina Agustina 10117087 B Ing Tugas II PDFLina AgustinaNo ratings yet
- Citation-230275240 RisDocument1 pageCitation-230275240 RisLina AgustinaNo ratings yet
- Citation-230275240 RisDocument1 pageCitation-230275240 RisLina AgustinaNo ratings yet
- Obat JantungDocument72 pagesObat JantungLina AgustinaNo ratings yet
- Obat JantungDocument72 pagesObat JantungLina AgustinaNo ratings yet
- Setyawan 2020 IOP Conf. Ser. Earth Environ. Sci. 468 012020Document8 pagesSetyawan 2020 IOP Conf. Ser. Earth Environ. Sci. 468 012020YendraNo ratings yet
- Common Pesticides in AgricultureDocument6 pagesCommon Pesticides in AgricultureBMohdIshaqNo ratings yet
- Stok 16 Juni 2023Document62 pagesStok 16 Juni 2023Icha FransiscaNo ratings yet
- Lista Medicamente OTC Conform Nomenclator ANM 17 Feb2020Document184 pagesLista Medicamente OTC Conform Nomenclator ANM 17 Feb2020Andreea PasolNo ratings yet
- Tim Mcnamara.: Mcnamara'S Country Store Rutherglen Rutherglen. Welcome !Document6 pagesTim Mcnamara.: Mcnamara'S Country Store Rutherglen Rutherglen. Welcome !api-25932006No ratings yet
- Write A Comment... : Cheerful NihilismDocument1 pageWrite A Comment... : Cheerful NihilismKatie bNo ratings yet
- Antibiotic Approval TimelineDocument1 pageAntibiotic Approval TimelineMartin CuellarNo ratings yet
- ClotrimazoleDocument2 pagesClotrimazoleSagar GuptaNo ratings yet
- PesticidesDocument12 pagesPesticidesNachiappan CN100% (2)
- TERMITICIDESAPPROVEDFORUSEINn ORTHc AROLINA6232014Document4 pagesTERMITICIDESAPPROVEDFORUSEINn ORTHc AROLINA6232014shiyanxiang0910No ratings yet
- Insecticides: S.No Technical Name Formulation Trade NamesDocument13 pagesInsecticides: S.No Technical Name Formulation Trade NamesRamkannan Parasumanna Chandrasekaran75% (16)
- RX Meds 2Document3 pagesRX Meds 2Carla PulgarNo ratings yet
- Mls 044: Clinical Bacteriology Session 9: Antimicrobial Agents - Mechanisms of Action and ResistanceDocument5 pagesMls 044: Clinical Bacteriology Session 9: Antimicrobial Agents - Mechanisms of Action and ResistanceJJ AngNo ratings yet
- Biopesticides Booklet FinalDocument40 pagesBiopesticides Booklet FinaldonbosskissNo ratings yet
- Pengaruh Penambahan Surfaktan Dan Waktu Turun HujaDocument10 pagesPengaruh Penambahan Surfaktan Dan Waktu Turun HujaSyaiful Anwar SiregarNo ratings yet
- Fs Item Master 06.08.21Document81 pagesFs Item Master 06.08.21Prem RathoreNo ratings yet
- 1 s2.0 S0924857922001455 MainDocument13 pages1 s2.0 S0924857922001455 MainRobert StryjakNo ratings yet
- Drone ApprovalDocument54 pagesDrone ApprovalAbhay SharmaNo ratings yet
- 17 Etest-Pricing v16 PDFDocument2 pages17 Etest-Pricing v16 PDFRapBoy TrinhNo ratings yet
- Liflet 6 Langkah Cuci TanganDocument3 pagesLiflet 6 Langkah Cuci TangangodeNo ratings yet
- Reaktor 1Document1 pageReaktor 1fadliNo ratings yet
- AntibioticsDocument10 pagesAntibioticsStevhenson PortacioNo ratings yet
- SS-Laktamski Antibiotici: Peroralni Parenteralni Penicilaza Rezistentni PeniciliniDocument5 pagesSS-Laktamski Antibiotici: Peroralni Parenteralni Penicilaza Rezistentni PeniciliniMali PrstNo ratings yet
- JAPON - Asparagus - 20230322061906Document9 pagesJAPON - Asparagus - 20230322061906Fiorella Alejandria YamucaNo ratings yet
- Antimicrobial Susceptibility TestingDocument3 pagesAntimicrobial Susceptibility TestingNoriz Ember DominguezNo ratings yet