You might also like
- Neuro EcDocument234 pagesNeuro EcFeynman2014100% (1)
- Mitsubishi Galant 4g63 Engine Repair ManualDocument29 pagesMitsubishi Galant 4g63 Engine Repair ManualMoaed Kanbar100% (1)
- Business Plan Hair DyeDocument12 pagesBusiness Plan Hair Dyercool_rahul0039341No ratings yet
- Better - Call - Saul - 4x10 WINNERDocument70 pagesBetter - Call - Saul - 4x10 WINNERMarcos Valdés GarridoNo ratings yet
- By Kerri Rivera, Kimberly Mcdaniel and Daniel Bender: Healing The Symptoms Known As Autism Second EditionDocument24 pagesBy Kerri Rivera, Kimberly Mcdaniel and Daniel Bender: Healing The Symptoms Known As Autism Second EditionMarilen De Leon EbradaNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- MIS DPCR IPCR July To December 2018 - Summary ListDocument14 pagesMIS DPCR IPCR July To December 2018 - Summary ListZyreen Kate BC100% (1)
- Magnesium Hydroxide (Milk of Magnesia)Document1 pageMagnesium Hydroxide (Milk of Magnesia)ENo ratings yet
- Reproductive System DrugsDocument100 pagesReproductive System DrugsR-jay Guevara100% (1)
- World Bank ReportDocument14 pagesWorld Bank Reportaditya_erankiNo ratings yet
- Psychedelic Drugs-A New Era in Psychiatry?Document9 pagesPsychedelic Drugs-A New Era in Psychiatry?PeterNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Norepinephrine Drug StudyDocument2 pagesNorepinephrine Drug StudyIrish LigayaNo ratings yet
- Zollinger Ellis Wps OfficeDocument15 pagesZollinger Ellis Wps OfficeAbhash MishraNo ratings yet
- Quiz Integumentary SystemDocument23 pagesQuiz Integumentary SystemLemuel CunananNo ratings yet
- AcetaminophenDocument2 pagesAcetaminophendrugcardref100% (1)
- Septic Abortion PDFDocument4 pagesSeptic Abortion PDFmariachrismayaniNo ratings yet
- Presentation on Chancroid: Bacterial STI Causes Painful Genital UlcersDocument12 pagesPresentation on Chancroid: Bacterial STI Causes Painful Genital UlcersBikash Sah0% (1)
- The Taste of Tradition: Submitted byDocument14 pagesThe Taste of Tradition: Submitted byvijay malikNo ratings yet
- POST PARTUM HEMORRHAGE: CAUSES, SIGNS, MANAGEMENTDocument38 pagesPOST PARTUM HEMORRHAGE: CAUSES, SIGNS, MANAGEMENTnyangaraNo ratings yet
- Endometrial Polyps: Irregular Menstrual BleedingDocument4 pagesEndometrial Polyps: Irregular Menstrual BleedingLuke ObusanNo ratings yet
- (Generic Name) ® Drotaverine 40mgDocument2 pages(Generic Name) ® Drotaverine 40mgSangar Sardar100% (1)
- ENT Drug StudyDocument3 pagesENT Drug StudyMcmac YangoNo ratings yet
- Manteux TestDocument25 pagesManteux TestEvaNatashaNo ratings yet
- 11 Nursing Management in Uterine (Endometrial) CancerDocument17 pages11 Nursing Management in Uterine (Endometrial) Cancerclaire yowsNo ratings yet
- FlagylDocument3 pagesFlagylAdrianne BazoNo ratings yet
- Caput SuccedaneumDocument2 pagesCaput SuccedaneumHerizko Kusuma100% (1)
- Streptokinase Mechanism and UsageDocument11 pagesStreptokinase Mechanism and UsageMalavika MadhuNo ratings yet
- CaffeineDocument2 pagesCaffeineSaini Malkeet100% (1)
- NEW ZEALAND DATA SHEET PETHIDINE TABLETSDocument13 pagesNEW ZEALAND DATA SHEET PETHIDINE TABLETSAnonymous NQDRERPcjNo ratings yet
- Briviact Film-Coated Tablets Summary of Product CharacteristicsDocument110 pagesBriviact Film-Coated Tablets Summary of Product CharacteristicsBendisDacicaNo ratings yet
- CAD - EBM September 2020 EditionDocument17 pagesCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiNo ratings yet
- Triamcinolone (Topical) - Drug InformationDocument5 pagesTriamcinolone (Topical) - Drug InformationMauricio Sv0% (1)
- Class Indications Available Dosage Form in The Hospital: AtosibanDocument2 pagesClass Indications Available Dosage Form in The Hospital: AtosibanDhanu GaysonsiriNo ratings yet
- Macrobid, Macrodantin (Nitrofurantoin) Dosing, Indications, Interactions, Adverse Effects, and More 2 PDFDocument2 pagesMacrobid, Macrodantin (Nitrofurantoin) Dosing, Indications, Interactions, Adverse Effects, and More 2 PDFNailis Sa'adahNo ratings yet
- ChemotherapyDocument35 pagesChemotherapynikhl saulNo ratings yet
- BromazepamDocument6 pagesBromazepamMariusNeicuNo ratings yet
- Diuretic Drugs PHMDocument36 pagesDiuretic Drugs PHMshenae3No ratings yet
- JINGCO - BSN 2-D - Module-6-Drug-StudyDocument16 pagesJINGCO - BSN 2-D - Module-6-Drug-StudyJashtine JingcoNo ratings yet
- Post Term PregnancyDocument12 pagesPost Term PregnancyRizky Putra Ismeldi100% (1)
- Pharma CardsDocument5 pagesPharma CardsazancheNo ratings yet
- Mesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidDocument4 pagesMesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidAnkan PalNo ratings yet
- Nodul Tiroidian Engleza PPT 2016Document36 pagesNodul Tiroidian Engleza PPT 2016Stefi GrNo ratings yet
- Drug StudyDocument2 pagesDrug StudyCen Janber CabrillosNo ratings yet
- BridionDocument18 pagesBridionEva Garcia MartinezNo ratings yet
- Alteplase Pharmacokinetics and Thrombolysis RisksDocument24 pagesAlteplase Pharmacokinetics and Thrombolysis Riskssatyagraha84No ratings yet
- MucosolvanDocument2 pagesMucosolvanAyah Paasa100% (1)
- Drug Order: Lonsurf (Trifluridine/TipiracilDocument3 pagesDrug Order: Lonsurf (Trifluridine/TipiracilKristine AcasioNo ratings yet
- Poisoning in ChildrenDocument11 pagesPoisoning in ChildrenAndriana HalfienNo ratings yet
- Seminar On MastectomyDocument8 pagesSeminar On Mastectomypooja singhNo ratings yet
- DrugStudy MetoclopramideDocument2 pagesDrugStudy MetoclopramideAshknee Khainna AlejoNo ratings yet
- Pyeloplasty (Anderson-Hynes)Document12 pagesPyeloplasty (Anderson-Hynes)HardiTariqHammaNo ratings yet
- Treating Tetanus: Support, Wound Care, AntitoxinsDocument11 pagesTreating Tetanus: Support, Wound Care, AntitoxinsFuad Adi PrasetyoNo ratings yet
- Acute Cholecystitis Ppt. DR Dilip S. RajpalDocument42 pagesAcute Cholecystitis Ppt. DR Dilip S. Rajpaldiliprajpal73100% (1)
- Anatomy and Pathophysiology of ProstrateDocument44 pagesAnatomy and Pathophysiology of Prostraterajan kumar100% (3)
- Preoperative Assessment of Diabetic PatientsDocument2 pagesPreoperative Assessment of Diabetic PatientsShilpa Pradhan100% (1)
- EzetimibeDocument3 pagesEzetimibeapi-3797941No ratings yet
- Seizure Disorders in ChildrenDocument22 pagesSeizure Disorders in ChildrenBheru LalNo ratings yet
- Metoclopramide (Reglan)Document1 pageMetoclopramide (Reglan)ENo ratings yet
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocument9 pagesDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoNo ratings yet
- Calcium Gluconate Injection for HypocalcemiaDocument9 pagesCalcium Gluconate Injection for HypocalcemiaLalrinchhanaNo ratings yet
- Integumentary System - Anatomy and PhysiologyDocument2 pagesIntegumentary System - Anatomy and PhysiologyHan CallejaNo ratings yet
- Levofloxacin Versus MoxifloxacinDocument3 pagesLevofloxacin Versus MoxifloxacinRina Trihandayani PutriNo ratings yet
- MTP Kit Medical Abortion GuideDocument8 pagesMTP Kit Medical Abortion GuidedoctorsujitNo ratings yet
- Manage Urinary Incontinence & RetentionDocument13 pagesManage Urinary Incontinence & RetentionDeniela Jamaicy HerbertNo ratings yet
- Prazosin Tablet (Prazosin)Document6 pagesPrazosin Tablet (Prazosin)Chenta Bulan MerinduNo ratings yet
- Flucloxacillin AFTcapssolnDocument6 pagesFlucloxacillin AFTcapssolnEliza ArmanNo ratings yet
- Daptomycin (Cubicin)Document1 pageDaptomycin (Cubicin)Adrianne BazoNo ratings yet
- Chronic Kidney Disease GuideDocument6 pagesChronic Kidney Disease GuideKyle Ü D. CunanersNo ratings yet
- Anticougulation in PregnancyDocument21 pagesAnticougulation in PregnancyLubna AliNo ratings yet
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- SECTION 03380 Post-Tensioned Concrete Rev 1Document30 pagesSECTION 03380 Post-Tensioned Concrete Rev 1Abdalrahman AntariNo ratings yet
- 2.factory Price - Alarm Accessories-Complete 20150325Document15 pages2.factory Price - Alarm Accessories-Complete 20150325FREE BUSINESS INTELLIGENCENo ratings yet
- 2 - FNCPDocument5 pages2 - FNCPIlda Lekka RequizaNo ratings yet
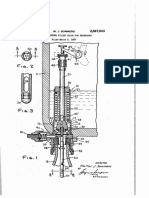
- Counter-pressure filler valve for beveragesDocument3 pagesCounter-pressure filler valve for beveragesbimalishaNo ratings yet
- LV CB Catalogue PDFDocument260 pagesLV CB Catalogue PDFBoobesh Kumar SekarNo ratings yet
- Fujitsu GeneralDocument51 pagesFujitsu GeneralZubair DarNo ratings yet
- Plane Bearings: Material Indicator Shape or SeriesDocument4 pagesPlane Bearings: Material Indicator Shape or SeriesJuan LoaizaNo ratings yet
- Department of The Navy Core Values CharterDocument1 pageDepartment of The Navy Core Values CharterShaun JohnsonNo ratings yet
- Polythionic Acid Stress Corrosion CrackingDocument2 pagesPolythionic Acid Stress Corrosion CrackingVajid MadathilNo ratings yet
- Importance and Uses of Medicinal Plants - An Overview: December 2016Document8 pagesImportance and Uses of Medicinal Plants - An Overview: December 2016safamanz001 safaNo ratings yet
- Analysis of Drinking Water Quality Parameters (A Case Study of Hanumangarh Town)Document8 pagesAnalysis of Drinking Water Quality Parameters (A Case Study of Hanumangarh Town)Editor IJTSRDNo ratings yet
- Dahong PalayDocument2 pagesDahong PalayAngela MontenegroNo ratings yet
- InfraTapp - Infra Tapp - Manual ENGDocument64 pagesInfraTapp - Infra Tapp - Manual ENGEliaNo ratings yet
- LC Used in ProteimicsDocument15 pagesLC Used in ProteimicsMandu ManNo ratings yet
- 4 WP 2013Document8 pages4 WP 2013TUTORKIMNo ratings yet
- Biomechinics PDFDocument8 pagesBiomechinics PDFImran KhanNo ratings yet
- Berca Engineering SUBMITTEDDocument20 pagesBerca Engineering SUBMITTEDJohandika FerbiantokoNo ratings yet
- STC Bec Wir Plu D 0209 01 PDFDocument10 pagesSTC Bec Wir Plu D 0209 01 PDFAdel MorsyNo ratings yet