You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Safety and Reference: Owner'S ManualDocument84 pagesSafety and Reference: Owner'S ManualjpmcorpNo ratings yet
- Immunopatologi Sepsis - DR Nur Farhanah SPPD K-PTIDocument29 pagesImmunopatologi Sepsis - DR Nur Farhanah SPPD K-PTIanita tri hastutiNo ratings yet
- Definisi-Klasifikasi EpilepsiDocument40 pagesDefinisi-Klasifikasi Epilepsianita tri hastuti100% (1)
- Scater DiagramDocument3 pagesScater Diagramanita tri hastutiNo ratings yet
- Cardiac Arrest 191108Document9 pagesCardiac Arrest 191108anita tri hastutiNo ratings yet
- Tx300 s3 OptionsDocument124 pagesTx300 s3 OptionsJorge Duran HerasNo ratings yet
- Anil Moris 9Document5 pagesAnil Moris 9Sudarsanam GollaNo ratings yet
- Traffic Signs Manual Chapter 05Document160 pagesTraffic Signs Manual Chapter 05Elliot MortonNo ratings yet
- Advanced Practice On Word Formation PDFDocument0 pagesAdvanced Practice On Word Formation PDFKhiem Vuong100% (1)
- Geologic TimeFossilsDocument1 pageGeologic TimeFossilsGracie ChingNo ratings yet
- Seminoma, BHP 3Document12 pagesSeminoma, BHP 3Deepika BananiNo ratings yet
- Exhibit Health, Safety, Security and Environmental Management Plan Requirement and StandardDocument113 pagesExhibit Health, Safety, Security and Environmental Management Plan Requirement and Standarddennisjuntak100% (1)
- Collaborative Lesson PlanDocument3 pagesCollaborative Lesson PlanMelissa QuinnNo ratings yet
- Aluminium Glass Composite Facade SystemDocument8 pagesAluminium Glass Composite Facade SystemIqrar HussainNo ratings yet
- Astm-D7596 - Iso 4406 PDFDocument7 pagesAstm-D7596 - Iso 4406 PDFPatricia MenaNo ratings yet
- The Low Down On Leather SustainabilityDocument5 pagesThe Low Down On Leather SustainabilitySetu BondhonNo ratings yet
- Extended Essay 4Document20 pagesExtended Essay 4thatoNo ratings yet
- Nutrient Cycling AND Climate Change: Kamala K. P202219Document12 pagesNutrient Cycling AND Climate Change: Kamala K. P202219KAMALA KNo ratings yet
- Bba Bba Batchno 70Document49 pagesBba Bba Batchno 70Upadhyay suchiNo ratings yet
- G0Vt - College of Nursing: SPMC, Agh BikanerDocument11 pagesG0Vt - College of Nursing: SPMC, Agh BikanerShubhra Sheoran100% (10)
- Bentone 38 - TDS - eDocument2 pagesBentone 38 - TDS - eDũng ĐỗNo ratings yet
- Design and Analysis of Column Structure For Jib CraneDocument6 pagesDesign and Analysis of Column Structure For Jib CraneGAURAVNo ratings yet
- 15-2 Cylinder Head Removing & Installing PDFDocument35 pages15-2 Cylinder Head Removing & Installing PDFmefisto06cNo ratings yet
- Improvement of Voltage Profile Through The Optimal Placement of FACTS Using L-Index MethodDocument5 pagesImprovement of Voltage Profile Through The Optimal Placement of FACTS Using L-Index MethodRavishankar KankaleNo ratings yet
- Sound Transit - 2022 Service Concepts Presentation - July 1, 2021Document12 pagesSound Transit - 2022 Service Concepts Presentation - July 1, 2021The UrbanistNo ratings yet
- 2006 2008 Cbf1000 A 1 General InformationDocument44 pages2006 2008 Cbf1000 A 1 General InformationMurariu IonutNo ratings yet
- The Social Determinants of Mental HealthDocument8 pagesThe Social Determinants of Mental Healthmelicruz14No ratings yet
- Wall Finishes PPT (1) (1) Taniya PDFDocument15 pagesWall Finishes PPT (1) (1) Taniya PDFRajaNo ratings yet
- MAIN Electrical Parts List: Design LOC Sec-Code DescriptionDocument12 pagesMAIN Electrical Parts List: Design LOC Sec-Code DescriptionAndroid Schematics and CircuitsNo ratings yet
- Biomarkers of Male Hypogonadism in Childhood and AdolescenceDocument13 pagesBiomarkers of Male Hypogonadism in Childhood and AdolescenceScott LoveNo ratings yet
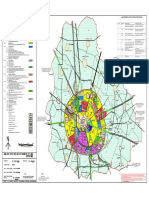
- Jhajjar Master PlanDocument1 pageJhajjar Master PlanMayank AhujaNo ratings yet
- SEL-2414 Transformer MonitorDocument3 pagesSEL-2414 Transformer MonitorMARTINCORTES1992100% (1)
- Certificate of Visual Examination and Dpi: Description of Equipment Billy Pugh X-904-4 Personnel Transfer DeviceDocument3 pagesCertificate of Visual Examination and Dpi: Description of Equipment Billy Pugh X-904-4 Personnel Transfer DeviceMichael OkwuwaNo ratings yet
- Nautical Flags and Their MeaningsDocument10 pagesNautical Flags and Their Meaningspeas_1030No ratings yet