You might also like
- Modeling in Food Microbiology: From Predictive Microbiology to Exposure AssessmentFrom EverandModeling in Food Microbiology: From Predictive Microbiology to Exposure AssessmentNo ratings yet
- NAP (Harry P.) PDFDocument29 pagesNAP (Harry P.) PDFaldyNo ratings yet
- Ppra Snars I Dr. DewiDocument93 pagesPpra Snars I Dr. DewiNilam atika sariNo ratings yet
- Materi DrharrypDocument38 pagesMateri DrharrypAnnisa Aisyha MalikNo ratings yet
- Program Pengendalian Resistensi Antimikroba: (PPRA) Di Rumah SakitDocument34 pagesProgram Pengendalian Resistensi Antimikroba: (PPRA) Di Rumah Sakitevy sari sutrisnaningsih100% (1)
- National Action Plan to Address AMR in IndonesiaDocument40 pagesNational Action Plan to Address AMR in IndonesiarosaliafriskaNo ratings yet
- Seminar AB Res FARMASI - Fix TitikNDocument74 pagesSeminar AB Res FARMASI - Fix TitikNLuthfiyyaNo ratings yet
- Risk Profile and Antimicrobial Susceptibility Pattern of Acinetobacter Baumanniiclinical Isolates in A Teaching Hospital in HyderabadDocument8 pagesRisk Profile and Antimicrobial Susceptibility Pattern of Acinetobacter Baumanniiclinical Isolates in A Teaching Hospital in HyderabadIJAR JOURNALNo ratings yet
- Program Pengendalian Resistensi Antimikroba Di Rumah SakitDocument23 pagesProgram Pengendalian Resistensi Antimikroba Di Rumah SakitYulia Wati Safitri SanjayaNo ratings yet
- Apollo PPT FinalDocument24 pagesApollo PPT Finalkrutarth shahNo ratings yet
- Amr Ppra Bethesda 2017 (DR Hari)Document29 pagesAmr Ppra Bethesda 2017 (DR Hari)Maya DamanikNo ratings yet
- Audit On Antibiotics Prescribing For Upper Respiratory Tract Infections in Primary Healthcare Facilities in Kedah (NMRR ID: NMRR-16-315-29590)Document34 pagesAudit On Antibiotics Prescribing For Upper Respiratory Tract Infections in Primary Healthcare Facilities in Kedah (NMRR ID: NMRR-16-315-29590)syamimiNo ratings yet
- AMR PPRA BETHESDA 2017 (DR Hari)Document26 pagesAMR PPRA BETHESDA 2017 (DR Hari)Susi WijayantiNo ratings yet
- Gyssen DDD MethodDocument39 pagesGyssen DDD MethodDewi RinakantiNo ratings yet
- Jurnal Mikro 1Document6 pagesJurnal Mikro 1Elang SudewaNo ratings yet
- Antibiotic Susceptibility Profile and Prevalence of AmpC Among Clinical Bacterial Isolates Obtained From Northwestern NigeriaDocument9 pagesAntibiotic Susceptibility Profile and Prevalence of AmpC Among Clinical Bacterial Isolates Obtained From Northwestern NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Global Problem Amrws Ppra Kars Ed CP Compressed - 998Document28 pagesGlobal Problem Amrws Ppra Kars Ed CP Compressed - 998budi darmantaNo ratings yet
- Antimicrobial Resistance in Indonesia: Causes, Impact and SolutionsDocument28 pagesAntimicrobial Resistance in Indonesia: Causes, Impact and SolutionsindriNo ratings yet
- Mendes 2014Document7 pagesMendes 2014Sergei VoychukNo ratings yet
- PF6400 - Antimicrobial StewardshipDocument63 pagesPF6400 - Antimicrobial StewardshipciaranNo ratings yet
- Shalamar Medical & Dental College, Lahore: Research TopicDocument12 pagesShalamar Medical & Dental College, Lahore: Research Topicdr ibtahajNo ratings yet
- Managing Antibiotic Resistance in cIAIDocument33 pagesManaging Antibiotic Resistance in cIAIAditya Pradana KNo ratings yet
- Global Problem AMR-NAP Dekon PONTIANAKDocument29 pagesGlobal Problem AMR-NAP Dekon PONTIANAKNurul MasyithahNo ratings yet
- HICC FOR NURSING EXCELLENCE-SMH SEPT 2018Document25 pagesHICC FOR NURSING EXCELLENCE-SMH SEPT 2018RakshaNo ratings yet
- Surveillance of MDRO in Indonesia HospitalsDocument29 pagesSurveillance of MDRO in Indonesia HospitalsElly Ssinouna ChubieNo ratings yet
- Dr. Arya Govinda - Management of OAB in ElderlyDocument36 pagesDr. Arya Govinda - Management of OAB in ElderlyCOVID RSHJNo ratings yet
- Antimicrobial Resistance in The Western Pacific Region: A Review of Surveillance and Health Systems ResponseDocument56 pagesAntimicrobial Resistance in The Western Pacific Region: A Review of Surveillance and Health Systems Response21NaiveNo ratings yet
- 06.Interpretation to Antibiograms WHONETDocument19 pages06.Interpretation to Antibiograms WHONETGilang KusdinarNo ratings yet
- 1 Hari - RSUA KPRA 3 Maret 2018 PDFDocument32 pages1 Hari - RSUA KPRA 3 Maret 2018 PDFElly Ssinouna ChubieNo ratings yet
- 1 Hari Rsua Kpra 3 Maret 2018Document32 pages1 Hari Rsua Kpra 3 Maret 2018Elly Ssinouna ChubieNo ratings yet
- Prevalence of Methicillinresistant Staphylococcus Aureus Andor Intermediate Susceptibility To Vancomycin Isolated From PDocument7 pagesPrevalence of Methicillinresistant Staphylococcus Aureus Andor Intermediate Susceptibility To Vancomycin Isolated From Pعالمي الجميلNo ratings yet
- Challenges of Achieving Viral Hepatitis Treatment Targets in EthiopiaDocument16 pagesChallenges of Achieving Viral Hepatitis Treatment Targets in EthiopiaEleni HagosNo ratings yet
- Study of Antibiotic-Resistance and Sensitivity Pattern in A Tertiary Care Teaching HospitalDocument8 pagesStudy of Antibiotic-Resistance and Sensitivity Pattern in A Tertiary Care Teaching HospitalIJAR JOURNALNo ratings yet
- DR Irwanto's SlidesDocument22 pagesDR Irwanto's SlidesAstria PermanaNo ratings yet
- Microbial Pathogenesis: SciencedirectDocument8 pagesMicrobial Pathogenesis: SciencedirectMaria Silvana AlvesNo ratings yet
- Shaotong Huai'an First People's Hospital, Nanjing Medical University, Huai'an, Jiangsu 223300, ChinaDocument4 pagesShaotong Huai'an First People's Hospital, Nanjing Medical University, Huai'an, Jiangsu 223300, ChinaFikarter ZukanevoNo ratings yet
- Jac-Antimicrobial ResistanceDocument12 pagesJac-Antimicrobial ResistanceKarina Dwi SwastikaNo ratings yet
- GeptodacinDocument6 pagesGeptodacinRubí YeverinoNo ratings yet
- Global Ssi Bethesda 2017 ABC (DR Hari)Document39 pagesGlobal Ssi Bethesda 2017 ABC (DR Hari)Maya DamanikNo ratings yet
- Juni 9 2023 AMR Di Indonesia Situasi Sekarang Dan Perkembangan PRA PERSIDocument51 pagesJuni 9 2023 AMR Di Indonesia Situasi Sekarang Dan Perkembangan PRA PERSImegaNo ratings yet
- Osteomyelitis JournalDocument7 pagesOsteomyelitis JournalAmalia Dwi AryantiNo ratings yet
- Multidrug Resistant Organisms in RSHS: Ida ParwatiDocument48 pagesMultidrug Resistant Organisms in RSHS: Ida Parwatiarief kurniawanNo ratings yet
- 23 Lakshmi Et AlDocument4 pages23 Lakshmi Et AleditorijmrhsNo ratings yet
- Journal of Infection: SciencedirectDocument8 pagesJournal of Infection: SciencedirectKarina Dwi SwastikaNo ratings yet
- CCO 2020 Contemporary Management of HIV Emerging Approaches DownloadableDocument52 pagesCCO 2020 Contemporary Management of HIV Emerging Approaches Downloadableluis hernandezNo ratings yet
- Resistance To Antifungal Agents: Mechanisms and Clinical ImpactDocument9 pagesResistance To Antifungal Agents: Mechanisms and Clinical ImpactAhmad BukhariNo ratings yet
- Jurnal Antibiotik 2Document11 pagesJurnal Antibiotik 2Achmad YunusNo ratings yet
- Kpra Persi Hospex Surabaya 2017 (Dr. Hari Paraton, Spog)Document22 pagesKpra Persi Hospex Surabaya 2017 (Dr. Hari Paraton, Spog)RSIA KENDANGSARI MERRNo ratings yet
- Antimicrobial Susceptibility Testing of Antimicrobial Peptides To Better Predict EfficacyDocument34 pagesAntimicrobial Susceptibility Testing of Antimicrobial Peptides To Better Predict EfficacyIkhva RiskianiNo ratings yet
- Increased Vancomycin Mics For Staphylococcus Aureus Clinical Isolates From A University Hospital During A 5-Year PeriodDocument4 pagesIncreased Vancomycin Mics For Staphylococcus Aureus Clinical Isolates From A University Hospital During A 5-Year Periodbarreiros8No ratings yet
- Knowledge, attitudes and practices of healthcare workers on needlestick injuriesDocument5 pagesKnowledge, attitudes and practices of healthcare workers on needlestick injuriesnik adrianiNo ratings yet
- The Revolution of Lateral Flow Assay in the Field of AMRDetectionDocument26 pagesThe Revolution of Lateral Flow Assay in the Field of AMRDetectionalbertNo ratings yet
- Webinar PPRADocument22 pagesWebinar PPRARizqi TitisNo ratings yet
- Antibiotic Guidelines - 2018 PDFDocument80 pagesAntibiotic Guidelines - 2018 PDFarnaldops333No ratings yet
- Amr Awareness Ppra Rs 2016abcdeDocument39 pagesAmr Awareness Ppra Rs 2016abcdeERA NORBIANINo ratings yet
- 3 Common Infectious Problems in PediatricsDocument102 pages3 Common Infectious Problems in PediatricsRajeshNo ratings yet
- Paso Corto 7 - Diagnostic Microbiology in Veterinary Dermatology-1Document10 pagesPaso Corto 7 - Diagnostic Microbiology in Veterinary Dermatology-1ABIGAIL AKEMI RODRIGUEZ CHAVEZNo ratings yet
- MRADocument17 pagesMRAmozhiarasuNo ratings yet
- Approach To Current Guidelines of SSI Prevention ABCDocument40 pagesApproach To Current Guidelines of SSI Prevention ABCPriyatnoNo ratings yet
- Mdro Global Amr 2018Document7 pagesMdro Global Amr 2018rifkidwianugrahNo ratings yet
- 100 Answers To Common English QuestionsDocument9 pages100 Answers To Common English Questionsflemus_1No ratings yet
- National Geographic USA - 01 2019Document145 pagesNational Geographic USA - 01 2019Minh ThuNo ratings yet
- New Monasticism: An Interspiritual Manifesto For Contemplative Life in The 21st CenturyDocument32 pagesNew Monasticism: An Interspiritual Manifesto For Contemplative Life in The 21st CenturyWorking With Oneness100% (8)
- NBCC Green ViewDocument12 pagesNBCC Green Views_baishyaNo ratings yet
- Skills Test Unit 1 Test A EmailDocument4 pagesSkills Test Unit 1 Test A EmailЛиза ОмельченкоNo ratings yet
- List of Registered Non Govt and Govt Secondary SchoolDocument200 pagesList of Registered Non Govt and Govt Secondary SchoolDennisEudes78% (9)
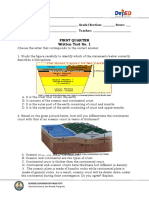
- Written Work 1 Q1 Science 10Document6 pagesWritten Work 1 Q1 Science 10JOEL MONTERDENo ratings yet
- Diseñadores Del Siglo XX - Las Figuras Clave Del Diseño y - Dormer, Peter - 1993 - Barcelona - Ceac - 9780747202684 - Anna's ArchiveDocument264 pagesDiseñadores Del Siglo XX - Las Figuras Clave Del Diseño y - Dormer, Peter - 1993 - Barcelona - Ceac - 9780747202684 - Anna's ArchiveSilvina RodríguezNo ratings yet
- PT JayatamaDocument67 pagesPT JayatamaAminadap. SIL.TNo ratings yet
- Introduction To Manufacturing ProcessesDocument64 pagesIntroduction To Manufacturing Processesnauman khanNo ratings yet
- Fabric Trademark and Brand Name IndexDocument15 pagesFabric Trademark and Brand Name Indexsukrat20No ratings yet
- IN SUNNY SPAIN, 1882-85: "My Country, My Love, My People, I Leave You Now, You Disappear, I Lose Sight of You"Document4 pagesIN SUNNY SPAIN, 1882-85: "My Country, My Love, My People, I Leave You Now, You Disappear, I Lose Sight of You"Mary Claire ComalaNo ratings yet
- Types of Companies Classified by Incorporation, Membership, Liability and ControlDocument11 pagesTypes of Companies Classified by Incorporation, Membership, Liability and ControlPrasad BulbuleNo ratings yet
- NCP GeriaDocument6 pagesNCP GeriaKeanu ArcillaNo ratings yet
- Forms of WillsDocument24 pagesForms of WillsJasNo ratings yet
- EasyGreen ManualDocument33 pagesEasyGreen ManualpitoupitouNo ratings yet
- Engineers Guide To Microchip 2018Document36 pagesEngineers Guide To Microchip 2018mulleraf100% (1)
- Module 4 Flexible Learning EnvironmentDocument2 pagesModule 4 Flexible Learning EnvironmentRyan Contratista GimarinoNo ratings yet
- Test Bank For American Pageant Volume 1 16th EditionDocument36 pagesTest Bank For American Pageant Volume 1 16th Editionzoonwinkfoxyj8100% (48)
- Water As A Weapon - Israel National NewsDocument11 pagesWater As A Weapon - Israel National NewsJorge Yitzhak Pachas0% (1)
- Bread and Pastry Production NC II 1st Edition 2016Document454 pagesBread and Pastry Production NC II 1st Edition 2016Brian Jade CadizNo ratings yet
- Our Lady of Consolation Orchestra InstrumentsDocument2 pagesOur Lady of Consolation Orchestra InstrumentsCelestian Valensario PaderangaNo ratings yet
- Australian Securities and Investments Commission V KingDocument47 pagesAustralian Securities and Investments Commission V KingCourtni HolderNo ratings yet
- The Tale of Sweet-Friend and Ali-NurDocument2 pagesThe Tale of Sweet-Friend and Ali-NurJomarie Siason Sumagpao100% (1)
- MarketNexus Editor: Teri Buhl Character LetterDocument2 pagesMarketNexus Editor: Teri Buhl Character LetterTeri BuhlNo ratings yet
- Recording of Dying DeclarationDocument6 pagesRecording of Dying DeclarationsarayusindhuNo ratings yet
- MgstreamDocument2 pagesMgstreamSaiful ManalaoNo ratings yet
- Holden Commodore Sedan VT To VZDocument6 pagesHolden Commodore Sedan VT To VZابو سعدNo ratings yet
- A Powerful Graphic Liquid Crystal Display: Column #47, March 1999 by Lon GlaznerDocument16 pagesA Powerful Graphic Liquid Crystal Display: Column #47, March 1999 by Lon GlaznerVijay P PulavarthiNo ratings yet
- VALUE BASED QUESTIONS FROM MATHEMATICS GRADE 10Document6 pagesVALUE BASED QUESTIONS FROM MATHEMATICS GRADE 10allyvluvyNo ratings yet