You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gastrulation in BirdsDocument20 pagesGastrulation in Birdskashif manzoor75% (4)
- Essentials of Orthognathic Surgery, 3eDocument14 pagesEssentials of Orthognathic Surgery, 3epaolacsuarezaNo ratings yet
- Duties and Qualities of A ButlerDocument6 pagesDuties and Qualities of A ButlerZiquerzMarkuz100% (1)
- Ongc Rig Equipment ManualDocument143 pagesOngc Rig Equipment Manualpablo92% (13)
- TheoriesDocument1 pageTheoriesThalia Milleña MiñuzaNo ratings yet
- 8 Things A Gynecologist Wants You To Stop Doing During Your Period CttoDocument3 pages8 Things A Gynecologist Wants You To Stop Doing During Your Period CttoThalia Milleña MiñuzaNo ratings yet
- Pigafetta's GROUP 1 BSN2BDocument9 pagesPigafetta's GROUP 1 BSN2BThalia Milleña MiñuzaNo ratings yet
- Pigafetta's GROUP 1 BSN2BDocument9 pagesPigafetta's GROUP 1 BSN2BThalia Milleña MiñuzaNo ratings yet
- Daily Checklist: YES YES YES YES YES X YESDocument47 pagesDaily Checklist: YES YES YES YES YES X YESEdmar TabinasNo ratings yet
- Sil 29-066 PDFDocument27 pagesSil 29-066 PDFblutonguyen0% (1)
- Sabrina Salsabila-Fkik PDFDocument178 pagesSabrina Salsabila-Fkik PDFHersan RNo ratings yet
- Biochemistry - Lipid ProfileDocument1 pageBiochemistry - Lipid ProfileHassan RazaNo ratings yet
- TCW241 Ethernet I O Module User Manual R4.2Document49 pagesTCW241 Ethernet I O Module User Manual R4.2Rodolfo OliveiraNo ratings yet
- ResearchDocument52 pagesResearchhisyam_muhd8No ratings yet
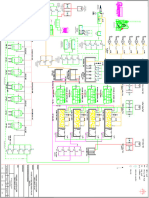
- P&ID-500 CMR-R1 (Original)Document1 pageP&ID-500 CMR-R1 (Original)Ahmed WagihNo ratings yet
- IntroductionDocument4 pagesIntroductionMarianna GurgutsovaNo ratings yet
- Part3 Icho 11 15 PDFDocument124 pagesPart3 Icho 11 15 PDFManuel GuilhermeNo ratings yet
- Pulmonary SurgeryDocument18 pagesPulmonary SurgeryShy PatelNo ratings yet
- SOCIALISATIONDocument8 pagesSOCIALISATIONAdityaNo ratings yet
- Example 14refrigerationDocument2 pagesExample 14refrigerationryan williamNo ratings yet
- Grading Rubric For DNA ModelDocument2 pagesGrading Rubric For DNA Modelcocosarang439No ratings yet
- GE XKcolumnsDocument12 pagesGE XKcolumnsJavi Profumo-Una Colegiata HumanaNo ratings yet
- Job Maldives Career Opportunities at Emerald Maldives Resort & SpaDocument1 pageJob Maldives Career Opportunities at Emerald Maldives Resort & SpaArlene Wilkinson Nia LucerousNo ratings yet
- Copper Alloy Guide EngDocument3 pagesCopper Alloy Guide EngRishi SharmaNo ratings yet
- p385 90Document35 pagesp385 90Edward MacDermidNo ratings yet
- Meritlist - Combined - 2015 29.08.2015 Final PDFDocument233 pagesMeritlist - Combined - 2015 29.08.2015 Final PDFAnshul AroraNo ratings yet
- Faculty 460 Eng 334 Kust20201 l2 p2 Paragraph WritingDocument20 pagesFaculty 460 Eng 334 Kust20201 l2 p2 Paragraph WritingMuhammad UsmanNo ratings yet
- 2011UCMC Trauma Care Q&ADocument2 pages2011UCMC Trauma Care Q&ASam CholkeNo ratings yet
- ØÁ L Nu T Uz È: Federal Negarit GazetaDocument17 pagesØÁ L Nu T Uz È: Federal Negarit GazetaHabtamu TadesseNo ratings yet
- SOR Chave Tipo Boia-1550-Sor-1Document20 pagesSOR Chave Tipo Boia-1550-Sor-1Costa SimesNo ratings yet
- Input Data Sheet For E-Class Record: Region Division School Name School Id School YearDocument18 pagesInput Data Sheet For E-Class Record: Region Division School Name School Id School YearRonie DacubaNo ratings yet
- Quick Reference Handbook: B-HLF A330-342 MSN 0113Document262 pagesQuick Reference Handbook: B-HLF A330-342 MSN 0113mikeNo ratings yet
- Application of Softener On 100% Cotton Dyed Fabric by Exhaust Method.Document4 pagesApplication of Softener On 100% Cotton Dyed Fabric by Exhaust Method.Naimul HasanNo ratings yet
- Experiment 6 - Linear Conduction PDFDocument13 pagesExperiment 6 - Linear Conduction PDFamir hamzahNo ratings yet