You might also like
- TetanusDocument29 pagesTetanusRyan JohnsonNo ratings yet
- Kepaniteraan Klinik RSD Mardi Waluyo Blitar - FK Unisma: Pembimbing: Dr. Utchu Tedja Mulya SP.BDocument35 pagesKepaniteraan Klinik RSD Mardi Waluyo Blitar - FK Unisma: Pembimbing: Dr. Utchu Tedja Mulya SP.BDada DoniNo ratings yet
- Torch: Jessica Santoso Moderator: Dr. Maimun ZA, M.Kes, SP - PKDocument79 pagesTorch: Jessica Santoso Moderator: Dr. Maimun ZA, M.Kes, SP - PKTommy KristantoNo ratings yet
- Constipation in ChildrenDocument34 pagesConstipation in Childrenabdisalaan hassanNo ratings yet
- Disaster Management Disaster Triage: Modul Introduction of Disaster Rumpun Ilmu Kesehatan - Universitas IndonesiaDocument100 pagesDisaster Management Disaster Triage: Modul Introduction of Disaster Rumpun Ilmu Kesehatan - Universitas IndonesiaindahNo ratings yet
- Tetanu S: Dr. MaslianiDocument74 pagesTetanu S: Dr. MaslianiHengky HanggaraNo ratings yet
- Congenital ToxoplasmosisDocument26 pagesCongenital ToxoplasmosisMichael WijayaNo ratings yet
- Congenital Cytomegalovirus Infection Clinical Features and DiagnosisDocument21 pagesCongenital Cytomegalovirus Infection Clinical Features and Diagnosisgomitas21No ratings yet
- K. Breaking Bad News (Dr. Iit)Document18 pagesK. Breaking Bad News (Dr. Iit)InggriOcviantiNingsihNo ratings yet
- Toxoplasma GondiiDocument29 pagesToxoplasma GondiiNagalingaNo ratings yet
- Modul Otologi Gangguan Nervus FasialisDocument65 pagesModul Otologi Gangguan Nervus FasialisHERIZALNo ratings yet
- Leprosy: An Overview of Pathophysiology: Disusun OlehDocument22 pagesLeprosy: An Overview of Pathophysiology: Disusun OlehDwi Endra Juli PraditoNo ratings yet
- CombinedDocument3 pagesCombinedSolape Akin-WilliamsNo ratings yet
- Referat CMVDocument33 pagesReferat CMVAndyn RobiolenyNo ratings yet
- Abdominal Lump-Nurcahyo Setiawan (2016) - 2Document95 pagesAbdominal Lump-Nurcahyo Setiawan (2016) - 2RobertOktaChandraNo ratings yet
- Brain Abcess: Ahmad Usama Wali House Servant Medical 1Document28 pagesBrain Abcess: Ahmad Usama Wali House Servant Medical 1Ahmad Talha WaliNo ratings yet
- Kuliah TETANUSDocument30 pagesKuliah TETANUSAraa AsukaNo ratings yet
- Infeksi NosokomialDocument29 pagesInfeksi NosokomialAlunaficha Melody KiraniaNo ratings yet
- Fraktur Tulang: Husnul Author Bag. Bedah RSUD CilacapDocument26 pagesFraktur Tulang: Husnul Author Bag. Bedah RSUD CilacapUmi YatunNo ratings yet
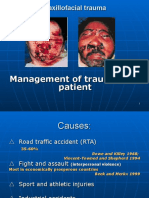
- Primary Management of Maxillofacial TraumaDocument34 pagesPrimary Management of Maxillofacial TraumafitsumNo ratings yet
- Askep Atresia EsophagusDocument18 pagesAskep Atresia EsophagusKhoLisoh Sae Anugrah100% (1)
- Jurnal Bedah PlastikDocument3 pagesJurnal Bedah PlastikBilly Shan LastKagerooboroNo ratings yet
- Worksheet SR-FAITHDocument4 pagesWorksheet SR-FAITHPPDSNeurologiAgustus 2021No ratings yet
- Kuliah Dinding AbdomenDocument41 pagesKuliah Dinding Abdomenelsa_111531No ratings yet
- Neonatal HypertensionDocument21 pagesNeonatal HypertensionMuhammad Ammar Abdul WahabNo ratings yet
- Brachial Plexus 1Document15 pagesBrachial Plexus 1Einstein JeromeNo ratings yet
- Course Study Guide: Occupational HealthDocument12 pagesCourse Study Guide: Occupational HealthGroup 12 Sofia HanaNo ratings yet
- Referat TetanusDocument51 pagesReferat TetanusDoddy Kusumah RonosulistyoNo ratings yet
- Compartment SyndromeDocument10 pagesCompartment SyndromerobbyNo ratings yet
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanNo ratings yet
- 2nd AnnouncementDocument2 pages2nd AnnouncementFauzan KurniawanNo ratings yet
- Spondylitis TBDocument33 pagesSpondylitis TBYohana KoliNo ratings yet
- Rupture Tendon Digiti III, IV, V Manus Sinistra Vulnus Laceratum Wrist Joint SinistraDocument13 pagesRupture Tendon Digiti III, IV, V Manus Sinistra Vulnus Laceratum Wrist Joint SinistraNubhy NubNo ratings yet
- Low Back Pain: Management Update: DR Dewanta Sembiring, SpsDocument46 pagesLow Back Pain: Management Update: DR Dewanta Sembiring, SpsYoke RetnaningpuriNo ratings yet
- Referat CTSDocument32 pagesReferat CTStrikurniati27No ratings yet
- GelafusalinfDocument5 pagesGelafusalinfToni Dafia PutraNo ratings yet
- White Island in The Red SeaDocument1 pageWhite Island in The Red SeaIndach RatnaNo ratings yet
- Review: Arthritis in LeprosyDocument6 pagesReview: Arthritis in LeprosyadlestariNo ratings yet
- Modul Utama OtologiDocument21 pagesModul Utama OtologikobexNo ratings yet
- Cara Baca RadiologiDocument25 pagesCara Baca RadiologiGumilang AryayudhaNo ratings yet
- Rhabdomyosarcoma Pedia Case ReportDocument36 pagesRhabdomyosarcoma Pedia Case ReportRem AlfelorNo ratings yet
- Upper Extremity Fracture - MKDocument85 pagesUpper Extremity Fracture - MKHawa AmbarwatiNo ratings yet
- CV Gatot Eamsc 2009Document3 pagesCV Gatot Eamsc 2009ShofaajiNo ratings yet
- Dr. Abdulmoneam Saleh Family Physician, JBFM, HSFM Dept. of Family & Community Medicine University of TabukDocument35 pagesDr. Abdulmoneam Saleh Family Physician, JBFM, HSFM Dept. of Family & Community Medicine University of TabukKholoud KholoudNo ratings yet
- Jurding PVDocument17 pagesJurding PVAnisaAyuningtyasNo ratings yet
- Acute Scrotum 231016 PDFDocument50 pagesAcute Scrotum 231016 PDFDany Dias100% (1)
- Leprosy: Pathogenesis Updated: ReviewDocument15 pagesLeprosy: Pathogenesis Updated: ReviewagneselimNo ratings yet
- Buttonhole DislocationDocument13 pagesButtonhole DislocationHanif Andhika WardhanaNo ratings yet
- I. Similar To Rounded Abdomen Only Greater. Anticipated in Pregnancy, Also Seen in Obesity, Ascites, and Other Conditions IIDocument3 pagesI. Similar To Rounded Abdomen Only Greater. Anticipated in Pregnancy, Also Seen in Obesity, Ascites, and Other Conditions IIroxanneNo ratings yet
- Meningitis: Prepared By: Mark Jansen Q. Abero Abby Pearl A. Allagadan Bsn-IiibDocument17 pagesMeningitis: Prepared By: Mark Jansen Q. Abero Abby Pearl A. Allagadan Bsn-IiibRodelyn Sequerra DariaNo ratings yet
- Daftar Nama Pendataan Pembimbing BedahDocument6 pagesDaftar Nama Pendataan Pembimbing Bedahegi lewisNo ratings yet
- Blok-22-Meningitis-Tuberkulosis Fakhrurrozi PratamaDocument16 pagesBlok-22-Meningitis-Tuberkulosis Fakhrurrozi PratamaFakhrurrozi PratamaNo ratings yet
- TN Fahrudin Vulnus ExcoriatumDocument10 pagesTN Fahrudin Vulnus Excoriatummonyet65No ratings yet
- DEN GU E: DengueDocument53 pagesDEN GU E: Denguerose ONo ratings yet
- Trauma Medulla SpinalisDocument79 pagesTrauma Medulla SpinalisiqiqiqiqiqNo ratings yet
- Cleft Lip and PalateDocument38 pagesCleft Lip and PalateHarry Sudarma AmersonNo ratings yet
- Neuralgia Post HerpetikDocument29 pagesNeuralgia Post HerpetikyheyenNo ratings yet
- Spleen: DR - Supriti Demonstrator Anatomy Deptt TMMC&RCDocument35 pagesSpleen: DR - Supriti Demonstrator Anatomy Deptt TMMC&RCBilal Yimam100% (1)
- Carpal Tunnel Syndrome JAAOS 2007 PDFDocument12 pagesCarpal Tunnel Syndrome JAAOS 2007 PDFStefano Pareschi PasténNo ratings yet
- Tetanus TutorialDocument27 pagesTetanus TutorialHerman SserubombwaNo ratings yet
- Guide SRW z2Document179 pagesGuide SRW z2Januar RezkyNo ratings yet
- 3745 PDFDocument6 pages3745 PDFJanuar RezkyNo ratings yet
- Oral Steroids For Resolution of Otitis Media With Effusion in Children (OSTRICH) : A Double-Blinded, Placebo-Controlled Randomised TrialDocument22 pagesOral Steroids For Resolution of Otitis Media With Effusion in Children (OSTRICH) : A Double-Blinded, Placebo-Controlled Randomised TrialJanuar RezkyNo ratings yet
- Platelet Glycoprotein Iib/Iiia Inhibition With Coronary Stenting For Acute Myocardial InfarctionDocument9 pagesPlatelet Glycoprotein Iib/Iiia Inhibition With Coronary Stenting For Acute Myocardial InfarctionJanuar RezkyNo ratings yet
- Continuing Medical Education: Fakultas Kedokteran Panitia Seminar Ilmiah NasionalDocument1 pageContinuing Medical Education: Fakultas Kedokteran Panitia Seminar Ilmiah NasionalJanuar RezkyNo ratings yet
- 4.2 MDS01 - Definition Table of The MDS Items - Ver0.94Document7 pages4.2 MDS01 - Definition Table of The MDS Items - Ver0.94AriniDwiLestariNo ratings yet
- TetanusDocument35 pagesTetanusJulie FurioNo ratings yet
- Toxoid VaccinesDocument2 pagesToxoid VaccinesKasandra Dawn Moquia Beriso100% (1)
- Tetanus - The DiseaseDocument6 pagesTetanus - The Diseasemanjunath mamathaNo ratings yet
- 10 List of Bacterial Infections MHEA NICOLE SALCEDO NEWDocument56 pages10 List of Bacterial Infections MHEA NICOLE SALCEDO NEWMhea Nicole SalcedoNo ratings yet
- Anaerobes and AnthraxDocument65 pagesAnaerobes and AnthraxGalih Maygananda PutraNo ratings yet
- Communicable Disease Nursing Test BankDocument11 pagesCommunicable Disease Nursing Test Bankdomingoramos685No ratings yet
- Clinical General ExaminationDocument26 pagesClinical General ExaminationAhmed AbdellaNo ratings yet
- Epidemioloske Karakteristike Tetanusa U HrvatskojDocument7 pagesEpidemioloske Karakteristike Tetanusa U HrvatskojRebecca BlackburnNo ratings yet
- MODULE 12-14 BOSH - With Pre-Final and Final ExamDocument23 pagesMODULE 12-14 BOSH - With Pre-Final and Final ExamEstelle May Beton AugustoNo ratings yet
- Nursing Practice IIDocument18 pagesNursing Practice IIstuffednurseNo ratings yet
- Medical TranslationDocument13 pagesMedical TranslationИванка СакареваNo ratings yet
- Tetanus in Animals - Summary of Knowledge Malinovská, Z., Čonková, E., Váczi, PDocument7 pagesTetanus in Animals - Summary of Knowledge Malinovská, Z., Čonková, E., Váczi, PSophieNo ratings yet
- Speaking Role Play CardsDocument28 pagesSpeaking Role Play CardsTheresa Fernandez50% (2)
- Communicable Disease Prevention and ControlDocument197 pagesCommunicable Disease Prevention and Controldennisjamesbartz100% (1)
- Nursing Practice II EdgeworthDocument9 pagesNursing Practice II EdgeworthRichard Ines Valino100% (1)
- Therapeutic Classification of Drugs Based On The Philippine National Drug FormularyDocument25 pagesTherapeutic Classification of Drugs Based On The Philippine National Drug FormularyJelight Faith Salero GachoNo ratings yet
- PE1Document23 pagesPE1abbynoreen2No ratings yet
- Salud Villanueva Vda de Bataclan VS Mariano Medina GR No. L-10126. October 22, 1957Document55 pagesSalud Villanueva Vda de Bataclan VS Mariano Medina GR No. L-10126. October 22, 1957dhadhagladysNo ratings yet
- 13 Areas of AssessmentDocument10 pages13 Areas of AssessmentNicole Anne TungolNo ratings yet
- Common DOG Bite DiseasesDocument3 pagesCommon DOG Bite DiseaseskhurramNo ratings yet
- Guidelines On TetanusDocument2 pagesGuidelines On Tetanusich4_28No ratings yet
- OB Nursing Test QuestionsDocument15 pagesOB Nursing Test QuestionsAileen Orjaliza Babanto100% (5)
- Pathophysiology of Tetanus: Clostridium Tetani BacteriaDocument3 pagesPathophysiology of Tetanus: Clostridium Tetani BacteriaSlepy chng100% (1)
- Epidemics After Natural Disasters PDFDocument5 pagesEpidemics After Natural Disasters PDFRafael CastilloNo ratings yet
- Pathophysiology of TetanusDocument2 pagesPathophysiology of TetanusAnitha SuprionoNo ratings yet
- Different Therepeutic Category of Drugs and Its Example Drug ProductsDocument8 pagesDifferent Therepeutic Category of Drugs and Its Example Drug ProductsGermie PosionNo ratings yet
- Foundations in Microbiology: TalaroDocument65 pagesFoundations in Microbiology: Talaromertx013No ratings yet
- Animal BitesDocument9 pagesAnimal BitesIlyes FerenczNo ratings yet
- Dog Bite 3Document2 pagesDog Bite 3ElvisNo ratings yet