You might also like
- Neoplasm On Bone and Soft Tissue MikoDocument151 pagesNeoplasm On Bone and Soft Tissue Mikoindra muhammadNo ratings yet
- An Approach To Malignant.7496050.PowerpointDocument19 pagesAn Approach To Malignant.7496050.PowerpointAndrei OlaruNo ratings yet
- Bone Tumor: Daniel A. (Orthopedic Surgeon)Document225 pagesBone Tumor: Daniel A. (Orthopedic Surgeon)mebrieNo ratings yet
- Benign Bone TumorsDocument31 pagesBenign Bone TumorsDr Afsar KhanNo ratings yet
- X-Ray: Most Useful of All ImagingDocument33 pagesX-Ray: Most Useful of All ImagingDinesh VeraNo ratings yet
- Dr. Ronald V. Munthe Spot SMF Bedah Rs UkiDocument50 pagesDr. Ronald V. Munthe Spot SMF Bedah Rs UkiOdilia Maria RahalusNo ratings yet
- Bone Tumours: Natasha Eleena Nor Maghfirah Hani Farhana Nur FadhilaDocument85 pagesBone Tumours: Natasha Eleena Nor Maghfirah Hani Farhana Nur FadhilaWan Nur AdilahNo ratings yet
- Musculoskelet Al Tumors: Rizal Daulay MD, Spot. MarsDocument98 pagesMusculoskelet Al Tumors: Rizal Daulay MD, Spot. MarsMuhammad AdityaNo ratings yet
- Neoplasm of Musculoskeletal Tissue: A GuideDocument48 pagesNeoplasm of Musculoskeletal Tissue: A Guidehello from the other sideNo ratings yet
- Tumours: Will Aston, Timothy Briggs, Louis SolomonDocument24 pagesTumours: Will Aston, Timothy Briggs, Louis SolomonShuvashishSunuwarNo ratings yet
- Septic ArthritisDocument94 pagesSeptic ArthritisCut Riska NovizaNo ratings yet
- Bone Tumor Diagnosis Approach BasicsDocument36 pagesBone Tumor Diagnosis Approach BasicsAnna Rinanta GintingNo ratings yet
- Bone TumorsDocument62 pagesBone TumorsEvan Permana PutraNo ratings yet
- BONE TUMOR ANALYSIS WITH X-RAYDocument73 pagesBONE TUMOR ANALYSIS WITH X-RAYAulia AlmiraNo ratings yet
- Bone Tumors 1Document44 pagesBone Tumors 1George josephNo ratings yet
- Tumors Around Knee in PediatricsDocument25 pagesTumors Around Knee in PediatricsMike RossNo ratings yet
- Tumors of Musculoskeletal: Tutorial Ortopaedic SurgeryDocument108 pagesTumors of Musculoskeletal: Tutorial Ortopaedic SurgeryfarisNo ratings yet
- Classification and Treatment of Bone TumorsDocument6 pagesClassification and Treatment of Bone TumorsRonald TejoprayitnoNo ratings yet
- Bone and Joint Neoplasm or TumorDocument49 pagesBone and Joint Neoplasm or Tumorendah rahmadaniNo ratings yet
- Bone and Joint TumoursDocument49 pagesBone and Joint TumoursMahmoud Abu Al Amrain100% (1)
- Basics Bone TumorsDocument104 pagesBasics Bone TumorsNitin BansalNo ratings yet
- Bone Tumors - DR OkunolaDocument36 pagesBone Tumors - DR OkunolaIdris Balasa IdrisNo ratings yet
- ABCDEF Approach To Radiographic Analysis of Bone TumorsDocument37 pagesABCDEF Approach To Radiographic Analysis of Bone Tumorsprashanth nagarajNo ratings yet
- Bone TumorsDocument40 pagesBone TumorsVisura PrabodNo ratings yet
- Chapter 12: Bone TumorsDocument14 pagesChapter 12: Bone TumorspoddataNo ratings yet
- MS TumorsDocument16 pagesMS TumorsASM MutahirNo ratings yet
- Slide Ajar B.2 Asdos 2015Document111 pagesSlide Ajar B.2 Asdos 2015Kumala DewiNo ratings yet
- Non-Odontogenic Tumor (Lecture)Document64 pagesNon-Odontogenic Tumor (Lecture)shabeelpn86% (7)
- Bone Tumors and Tumor-Like LesionsDocument22 pagesBone Tumors and Tumor-Like LesionsOswin Caicedo100% (1)
- Bone Tumor FinalDocument156 pagesBone Tumor Finalavni_stormNo ratings yet
- Bone tm3Document57 pagesBone tm3ZakiyahulfahdwNo ratings yet
- 6.musculoskeletal TumorsDocument110 pages6.musculoskeletal Tumorslina jamalNo ratings yet
- 3 - Imaging Hand Tumours FESSHDocument37 pages3 - Imaging Hand Tumours FESSHProfesseur Christian DumontierNo ratings yet
- Bone Tumors and Tumorlike Conditions: Analysis With Conventional RadiographyDocument73 pagesBone Tumors and Tumorlike Conditions: Analysis With Conventional RadiographyViskaNo ratings yet
- Bone Destruction and TypeDocument51 pagesBone Destruction and TypeHuyền LêNo ratings yet
- Bone Tumor Radiographic Findings: Key Signs of Benign vs MalignantDocument23 pagesBone Tumor Radiographic Findings: Key Signs of Benign vs MalignantFarizka Dwinda HNo ratings yet
- Bone Tumours: Mohamad Bayu SahadewaDocument31 pagesBone Tumours: Mohamad Bayu SahadewaDwi SarwindaNo ratings yet
- Classification and Imaging Features of Primary Bone TumorsDocument5 pagesClassification and Imaging Features of Primary Bone TumorsnmahpbooksNo ratings yet
- Booooooone Tumors REFERATDocument47 pagesBooooooone Tumors REFERATNurlaila IshaqNo ratings yet
- Foot and Ankle Tumor Radiographic FeaturesDocument9 pagesFoot and Ankle Tumor Radiographic FeaturesShazeb RizviNo ratings yet
- Malignant Tumors FESSHDocument40 pagesMalignant Tumors FESSHProfesseur Christian DumontierNo ratings yet
- Tumors of Bone-2Document33 pagesTumors of Bone-2Jackline nyawiraNo ratings yet
- Bone Tumours: - Jeffrey Pradeep RajDocument42 pagesBone Tumours: - Jeffrey Pradeep RajjeffreyprajNo ratings yet
- Di - Bone Tumor Presentation - 9-27-07Document12 pagesDi - Bone Tumor Presentation - 9-27-07widyaanggariniNo ratings yet
- Bone Tumor Seminar: Types & ManagementDocument80 pagesBone Tumor Seminar: Types & ManagementPATHMAPRIYA GANESANNo ratings yet
- Short Version Malignant Bone LesionsDocument57 pagesShort Version Malignant Bone LesionsAfNo ratings yet
- Bone TumorsDocument6 pagesBone Tumorsa179360No ratings yet
- Tumours: Apley 9th Ed p.187-223Document66 pagesTumours: Apley 9th Ed p.187-223Helmi IsmunandarNo ratings yet
- Bone Tumor Presentation - 9-27-07Document12 pagesBone Tumor Presentation - 9-27-07Febbi Iral Bin AgusNo ratings yet
- Bone Tumors: Benign Tumor Malignant TumorDocument5 pagesBone Tumors: Benign Tumor Malignant TumorManish ShresthaNo ratings yet
- Bone TumourDocument78 pagesBone TumourGaluh Kresna BayuNo ratings yet
- Seminar W4 - Bone & Soft Tissue TumoursDocument123 pagesSeminar W4 - Bone & Soft Tissue TumoursUN EPNo ratings yet
- Benign Bone TumoursDocument13 pagesBenign Bone TumoursAnisah MahmudahNo ratings yet
- Chondrosarcoma 1Document74 pagesChondrosarcoma 1IceBearNo ratings yet
- Management of Benign Bone Neoplasm by Eyecherry 3 - 2 (Autosaved)Document51 pagesManagement of Benign Bone Neoplasm by Eyecherry 3 - 2 (Autosaved)Osifo EmmanuelNo ratings yet
- Tumors of MusculoskeletalDocument7 pagesTumors of MusculoskeletalodiliajessicanpviaNo ratings yet
- Patologi Anatomi Kelainan MuskuloskeletalDocument38 pagesPatologi Anatomi Kelainan Muskuloskeletalmuthia saniNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- Discover Over 70 Player Classes and RacesDocument1 pageDiscover Over 70 Player Classes and RacesFred FrançaNo ratings yet
- Oxford SuprEsser ManualDocument34 pagesOxford SuprEsser ManualaaaNo ratings yet
- Maximizing Area and Minimizing Costs with CalculusDocument18 pagesMaximizing Area and Minimizing Costs with Calculusanon_218576188No ratings yet
- API Calcs Rev1 (Version 2)Document112 pagesAPI Calcs Rev1 (Version 2)Jake Sparrow100% (1)
- Training ManualDocument41 pagesTraining Manualemiliow_1100% (3)
- 05.G. Before Takeoff CheckDocument4 pages05.G. Before Takeoff CheckUDAYAPRAKASH RANGASAMYNo ratings yet
- Mec 323Document68 pagesMec 323VINAY B.SNo ratings yet
- BMK PDFDocument8 pagesBMK PDFHuỳnh Minh SángNo ratings yet
- Orac Charts - BuenisimoDocument92 pagesOrac Charts - BuenisimosanthigiNo ratings yet
- English HL Grade 8 Language Exam Nov 2017 MEMODocument12 pagesEnglish HL Grade 8 Language Exam Nov 2017 MEMOThegn's PicklesNo ratings yet
- Akbh PSK (V), TRBH As Y: AdhimokṣADocument8 pagesAkbh PSK (V), TRBH As Y: AdhimokṣA张晓亮No ratings yet
- Factors to Consider in Reactor Design for Industrial ProcessesDocument3 pagesFactors to Consider in Reactor Design for Industrial Processesuma villashini100% (2)
- Solar Collectors Final WordDocument14 pagesSolar Collectors Final WordVaibhav Vithoba NaikNo ratings yet
- RTWP OptimisationHanFeedbackDocument31 pagesRTWP OptimisationHanFeedbackSeth Mawuli Dedzoe100% (1)
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument21 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For Scientistsnonzero15No ratings yet
- Maersk QuestionnaireDocument43 pagesMaersk QuestionnaireSahil SharmaNo ratings yet
- Israel Is The MessIahDocument288 pagesIsrael Is The MessIahTeerayoot NoidaNo ratings yet
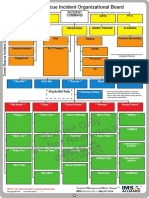
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- SilverDocument16 pagesSilversharma_shruti0% (1)
- Calculation of Carbon Footprint: HouseDocument3 pagesCalculation of Carbon Footprint: HouseUmut ÇağırganNo ratings yet
- 9th Mole Concept and Problems Based On PDFDocument2 pages9th Mole Concept and Problems Based On PDFMintu KhanNo ratings yet
- Worthy - Elevation WorshipDocument1 pageWorthy - Elevation WorshipSabine J.100% (1)
- Miniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDocument4 pagesMiniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDenis CarlosNo ratings yet
- Module 2 Chem 1Document25 pagesModule 2 Chem 1melissa cabreraNo ratings yet
- Growth, Stagnation or Decline? Agfficulturalproductm'Iy in British IndiaDocument290 pagesGrowth, Stagnation or Decline? Agfficulturalproductm'Iy in British IndiaHarshadeep BiswasNo ratings yet
- Friends of Hursley School: Late Summer NewsletterDocument6 pagesFriends of Hursley School: Late Summer Newsletterapi-25947758No ratings yet
- Buckling TestDocument11 pagesBuckling Testsharusli100% (1)
- PR900 Operator ManualDocument21 pagesPR900 Operator ManualAlan TanNo ratings yet
- Caelus TT - Caelus Product TrainingDocument93 pagesCaelus TT - Caelus Product TrainingYader Daniel Ortiz CerdaNo ratings yet
- Mini ProjectDocument6 pagesMini Projectirene0% (1)