You might also like
- Microbial GrowthDocument12 pagesMicrobial GrowthJosé MolinerosNo ratings yet
- Notes Pathoma Webinar PDF PDFDocument84 pagesNotes Pathoma Webinar PDF PDFNosheen Hafeez100% (1)
- CH1 Path D&R AgamDocument34 pagesCH1 Path D&R Agam062100% (1)
- Biology Cornell Notes HWDocument3 pagesBiology Cornell Notes HWapi-330055989No ratings yet
- 02.07.4 Cell Injury I FINALDocument52 pages02.07.4 Cell Injury I FINALNawlannieNo ratings yet
- 1 - PATHOLOGY - Cellular Injury, Cellular Adaptation, and Cell Death LectureDocument25 pages1 - PATHOLOGY - Cellular Injury, Cellular Adaptation, and Cell Death Lectureregeti bhargavNo ratings yet
- HS 202 - 1Document5 pagesHS 202 - 1trina santiagoNo ratings yet
- 2.2. Cell Adaptation, Injury and DeathDocument53 pages2.2. Cell Adaptation, Injury and Deathakoeljames8543No ratings yet
- 0828 Introduction and Cellular InjuryDocument74 pages0828 Introduction and Cellular Injury李宜芳No ratings yet
- Adapted Study Guide Cellular AdaptationDocument2 pagesAdapted Study Guide Cellular AdaptationmegNo ratings yet
- Cellular Adaptation and AccumulationDocument4 pagesCellular Adaptation and AccumulationMariel AsisNo ratings yet
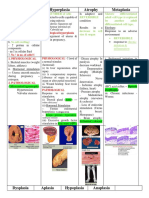
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument24 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- 5) Degeneration, Necrosis and GangreneDocument72 pages5) Degeneration, Necrosis and GangreneMadhulikaNo ratings yet
- 2 CELL INJURY AND CELL DEATH Reviewer 2Document4 pages2 CELL INJURY AND CELL DEATH Reviewer 2manuelNo ratings yet
- PathologyDocument117 pagesPathologyDrChauhanNo ratings yet
- Cellular Adaptation - 2022Document49 pagesCellular Adaptation - 2022Leo Lucifer 104No ratings yet
- Cell Injury & AdaptationDocument22 pagesCell Injury & AdaptationUmam LoyalNo ratings yet
- Adaptation and Injury of Cell: Extracellular StressesDocument8 pagesAdaptation and Injury of Cell: Extracellular StressesCrystal GazingNo ratings yet
- Adaptations, Cell Injury, Cell Death: Dr. Ashish Jawarkar, MDDocument77 pagesAdaptations, Cell Injury, Cell Death: Dr. Ashish Jawarkar, MDEdsel Ian S. FuentesNo ratings yet
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- HomeostasisDocument16 pagesHomeostasiskimkaigel6No ratings yet
- Andrea Tonelli: MBCHB (Uct) 2018Document167 pagesAndrea Tonelli: MBCHB (Uct) 2018BasitNo ratings yet
- Cell Adaptation, Injury and DeathDocument91 pagesCell Adaptation, Injury and DeathAmera ElsayedNo ratings yet
- Cell InjuryDocument39 pagesCell InjuryZainul Iman Abdul MalekNo ratings yet
- 1P Patho Lab ReviewerDocument95 pages1P Patho Lab ReviewerAakash NihalaniNo ratings yet
- Patho Written 108Document11 pagesPatho Written 108Nina Khaled YoussefNo ratings yet
- Chapter 1 Cell InjuryDocument21 pagesChapter 1 Cell Injuryhenna patelNo ratings yet
- Pathology DKDocument367 pagesPathology DKAshok DaukiyaNo ratings yet
- Cellular Adaptations and Cell DeathDocument4 pagesCellular Adaptations and Cell DeathShuaib SiddiquiNo ratings yet
- SHS 301 Lect-2Document29 pagesSHS 301 Lect-2AAZEEN ALINo ratings yet
- Histopathology - Lec Prelim 1Document43 pagesHistopathology - Lec Prelim 1Jean Calubag CatalanNo ratings yet
- Plenary 2: "Yang Tersembunyi"Document92 pagesPlenary 2: "Yang Tersembunyi"Fathoni akbarNo ratings yet
- Cell InjuryDocument22 pagesCell InjuryKainat LatifNo ratings yet
- PathologyDocument119 pagesPathologyDavid VijayNo ratings yet
- CellularAdaptation Injury and Death - General OverviewDocument13 pagesCellularAdaptation Injury and Death - General OverviewlydNo ratings yet
- Cellular Adaptation and InjuryDocument6 pagesCellular Adaptation and InjuryPrince D. JacobNo ratings yet
- Cell Injury 3 Apoptosis and AutophagyDocument17 pagesCell Injury 3 Apoptosis and Autophagykhaledbarham.2003No ratings yet
- Cell Adaptation & Response To Injury by NikitaDocument3 pagesCell Adaptation & Response To Injury by NikitaMedical Student NotesNo ratings yet
- Dist of Growth 1 2023 LectureDocument60 pagesDist of Growth 1 2023 LecturejaidenrmNo ratings yet
- Conference 1Document71 pagesConference 1titusonNo ratings yet
- Difference BLN Hypertropy &atropyDocument2 pagesDifference BLN Hypertropy &atropyFu'e AbdumalikNo ratings yet
- Patho SGD 1 PDFDocument5 pagesPatho SGD 1 PDFOella CabangonNo ratings yet
- Patho MidtermsDocument8 pagesPatho Midtermswieka mawieNo ratings yet
- Cell DeathDocument6 pagesCell DeathClaraNo ratings yet
- Histopathology NotesDocument12 pagesHistopathology NotesLeandro Miguel TongolNo ratings yet
- CA RevisedDocument19 pagesCA RevisedmarkyboiNo ratings yet
- Cellular Adaptations and Responses to Stress and DamageDocument50 pagesCellular Adaptations and Responses to Stress and DamageKimberly AnnNo ratings yet
- PathologyDocument217 pagesPathologyhindrina8No ratings yet
- Cellular Adaptation and NecrosisDocument30 pagesCellular Adaptation and NecrosisHilary Dianne TutoNo ratings yet
- Apoptosis & Necrosis: Suad Omar NafiDocument46 pagesApoptosis & Necrosis: Suad Omar Nafisoad onafiNo ratings yet
- Cell Injury, Cell Death, AdaptationDocument64 pagesCell Injury, Cell Death, Adaptationtiararudianti20No ratings yet
- Cell Injury (Dr. Sriwidyani)Document75 pagesCell Injury (Dr. Sriwidyani)galuh dharmapatniNo ratings yet
- Chapter Two Tissue InjuryDocument38 pagesChapter Two Tissue Injuryapi-19916399No ratings yet
- HM/CH-1/L-8: Morphology of Cell InjuryDocument11 pagesHM/CH-1/L-8: Morphology of Cell Injuryyashika pkkNo ratings yet
- Cellular Injury and AdaptationsDocument145 pagesCellular Injury and AdaptationsAjmal RockzzNo ratings yet
- Cellular AdaptationsDocument29 pagesCellular AdaptationsZainul Iman Abdul MalekNo ratings yet
- Pathology01 CellDeath Inflammation RepairDocument140 pagesPathology01 CellDeath Inflammation RepairMiguel AranaNo ratings yet
- Cellular Adaptations in Growth and DifferentiationDocument32 pagesCellular Adaptations in Growth and Differentiationvinoedhnaidu_rajagopalNo ratings yet
- Pathology FDocument42 pagesPathology FAryan SahNo ratings yet
- Necrosis and Cellualr AdaptationDocument56 pagesNecrosis and Cellualr AdaptationEs SarveshNo ratings yet
- Cell Injury, Cell Death, and Adaptations: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocument27 pagesCell Injury, Cell Death, and Adaptations: Dr. I Made Naris Pujawan, M.Biomed, SP - PAlindaNo ratings yet
- Biochemistry Course Outline FinalDocument3 pagesBiochemistry Course Outline FinalMiriam JonesNo ratings yet
- Chapter 28 AdrenocorticoidsDocument36 pagesChapter 28 AdrenocorticoidsCapuNo ratings yet
- Mitochondrial Respiratory Chain Disorders I Mitochondrial DNADocument6 pagesMitochondrial Respiratory Chain Disorders I Mitochondrial DNAAngie CeronNo ratings yet
- Eukaryotic TranslationDocument24 pagesEukaryotic Translationtariqul13017No ratings yet
- Molecular Basis of InheritanceDocument42 pagesMolecular Basis of InheritanceJayashree JanarthanamNo ratings yet
- 9 Mid Term Xam Paper 2020Document2 pages9 Mid Term Xam Paper 2020om guptaNo ratings yet
- Chapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFDocument9 pagesChapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFChethranNo ratings yet
- The Muscular System: Lecture Presentation by Patty Bostwick-Taylor Florence-Darlington Technical CollegeDocument35 pagesThe Muscular System: Lecture Presentation by Patty Bostwick-Taylor Florence-Darlington Technical CollegeTrisha100% (3)
- pgl3 Luciferase Reporter Vectors Protocol PDFDocument31 pagespgl3 Luciferase Reporter Vectors Protocol PDFSr. RZNo ratings yet
- FACILITATED DIFFUSIONDocument2 pagesFACILITATED DIFFUSIONCarlo CondeNo ratings yet
- Lecture 1 - Animal Cell Types and TissuesDocument67 pagesLecture 1 - Animal Cell Types and TissuesEthel Gerardo PabloNo ratings yet
- Lecture2 GranulopoiesisDocument9 pagesLecture2 GranulopoiesisAfifa Prima GittaNo ratings yet
- Melanocytes: The Skin's Pigment Producing CellsDocument3 pagesMelanocytes: The Skin's Pigment Producing Cellsأحمد المسيريNo ratings yet
- Hint & Sheet Your Hard Work Leads To Strong Foundation: Pre-Nurture: Class - IxDocument5 pagesHint & Sheet Your Hard Work Leads To Strong Foundation: Pre-Nurture: Class - IxAmit RoutNo ratings yet
- Fish immune system and vaccines-Springer (2022)-1Document293 pagesFish immune system and vaccines-Springer (2022)-1Rodolfo Velazco100% (1)
- Photosynthesis and Cellular Respiration LabDocument11 pagesPhotosynthesis and Cellular Respiration Labapi-358704014No ratings yet
- Science 7 Chapter 1 - Cells 1.3-1.4Document13 pagesScience 7 Chapter 1 - Cells 1.3-1.4Hương Minh Phạm QuinnNo ratings yet
- 5 Hpe Axis Sum21 StudentDocument7 pages5 Hpe Axis Sum21 StudentRAQUEL WINECKNo ratings yet
- Pmby1101 Lecture10 2013Document10 pagesPmby1101 Lecture10 2013Hdlbr RhaNo ratings yet
- Biopharma Expression Systems 080926Document340 pagesBiopharma Expression Systems 080926Sungsik ParkNo ratings yet
- Effects of Electromagnetic Field On The Development of Chick Embryo: An in Vivo Study - IntechOpenDocument2 pagesEffects of Electromagnetic Field On The Development of Chick Embryo: An in Vivo Study - IntechOpensokhna may seyeNo ratings yet
- January 2009 QP - Unit 1 Edexcel Biology A-LevelDocument24 pagesJanuary 2009 QP - Unit 1 Edexcel Biology A-LevelFatma ZorluNo ratings yet
- Lec-3-Dna Replication, Transcription, and TranslationDocument11 pagesLec-3-Dna Replication, Transcription, and TranslationGreatel Elijah TorregosaNo ratings yet
- Lecture 9 & 10 - Endomembrane System I & IIDocument8 pagesLecture 9 & 10 - Endomembrane System I & IILujainNo ratings yet
- Dna Extraction From Bananas: Group 4 Bio-Drrr-MDocument16 pagesDna Extraction From Bananas: Group 4 Bio-Drrr-MRevirae Camil AriolaNo ratings yet
- EritropoesisDocument15 pagesEritropoesisFitriyani Dewi SuwandhiNo ratings yet
- Thyroid & Parathyroid HormonesDocument53 pagesThyroid & Parathyroid Hormonesrehmanmughal87654No ratings yet
- Introduction to Neurons and Ion ChannelsDocument7 pagesIntroduction to Neurons and Ion ChannelsKamalNo ratings yet