You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Manual Vineland II PDFDocument346 pagesManual Vineland II PDFAdryAriza85% (61)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- J. William Lloyd - The Karezza Method PDFDocument32 pagesJ. William Lloyd - The Karezza Method PDFmmm100% (1)
- Urinary Tract InfectionsDocument56 pagesUrinary Tract InfectionsIoana CozmaNo ratings yet
- CBT Case Study PresentationDocument12 pagesCBT Case Study Presentationstefiano100% (1)
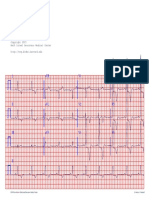
- Caz 11 PDFDocument1 pageCaz 11 PDFIoana CozmaNo ratings yet
- Carol Davila Pathophysiology NotesDocument7 pagesCarol Davila Pathophysiology NotesGiorgos Doukas KaranasiosNo ratings yet
- Caz 22 PDFDocument1 pageCaz 22 PDFIoana CozmaNo ratings yet
- Caz 92 PDFDocument1 pageCaz 92 PDFIoana CozmaNo ratings yet
- Caz 12 PDFDocument1 pageCaz 12 PDFIoana CozmaNo ratings yet
- Caz 83 PDFDocument1 pageCaz 83 PDFIoana CozmaNo ratings yet
- Caz 13 PDFDocument1 pageCaz 13 PDFIoana CozmaNo ratings yet
- Complications PDFDocument79 pagesComplications PDFIoana CozmaNo ratings yet
- Caz 5 PDFDocument1 pageCaz 5 PDFIoana CozmaNo ratings yet
- Caz 22 PDFDocument1 pageCaz 22 PDFIoana CozmaNo ratings yet
- Caz 53 PDFDocument1 pageCaz 53 PDFIoana CozmaNo ratings yet
- LEC 03 - Pituitary Tumours PDFDocument54 pagesLEC 03 - Pituitary Tumours PDFIoana CozmaNo ratings yet
- 03 - Thorax 2 PDFDocument93 pages03 - Thorax 2 PDFIoana CozmaNo ratings yet
- Caz 14 PDFDocument1 pageCaz 14 PDFIoana CozmaNo ratings yet
- LEC 04 - Hypo - Hyperthyroidism PDFDocument115 pagesLEC 04 - Hypo - Hyperthyroidism PDFIoana CozmaNo ratings yet
- Caz 17 PDFDocument1 pageCaz 17 PDFIoana CozmaNo ratings yet
- Caz 240 PDFDocument1 pageCaz 240 PDFIoana CozmaNo ratings yet
- Definitions PDFDocument7 pagesDefinitions PDFIoana CozmaNo ratings yet
- General Survey (Lecture 1)Document91 pagesGeneral Survey (Lecture 1)Ioana CozmaNo ratings yet
- Introduction PDFDocument21 pagesIntroduction PDFIoana CozmaNo ratings yet
- LEC 05 - Growth - Puberty DisordersDocument58 pagesLEC 05 - Growth - Puberty DisordersIoana CozmaNo ratings yet
- LEC 04 - Hypo - Hyperthyroidism PDFDocument115 pagesLEC 04 - Hypo - Hyperthyroidism PDFIoana CozmaNo ratings yet
- Thyroid CancerDocument28 pagesThyroid CancerIoana CozmaNo ratings yet
- Infectious Diseases. Etiology PDFDocument76 pagesInfectious Diseases. Etiology PDFIoana CozmaNo ratings yet
- LEC 03 - Pituitary TumoursDocument54 pagesLEC 03 - Pituitary TumoursIoana CozmaNo ratings yet
- LEC 02 - Hypothalamus - Hypopituitarism PDFDocument31 pagesLEC 02 - Hypothalamus - Hypopituitarism PDFIoana CozmaNo ratings yet
- LEC 01 - Principles of EndocrinologyDocument44 pagesLEC 01 - Principles of EndocrinologyIoana Cozma100% (1)
- Lecture 2B - Fetal Presentations and Positions During DeliveryDocument40 pagesLecture 2B - Fetal Presentations and Positions During DeliveryIoana CozmaNo ratings yet
- Apr W1,2Document6 pagesApr W1,2Toànn ThiệnnNo ratings yet
- Manahaw Elementary School Child Protection PolicyDocument3 pagesManahaw Elementary School Child Protection PolicyRenelyn Rodrigo SugarolNo ratings yet
- Organizing Is Good For Mental HealthDocument2 pagesOrganizing Is Good For Mental Healthamos wabwileNo ratings yet
- Reinforcement Theory of MotivationDocument10 pagesReinforcement Theory of Motivationimdad ullahNo ratings yet
- Philosophy Term PaperDocument23 pagesPhilosophy Term PaperMvieNo ratings yet
- The Children's Code Bill, 2022 FinalDocument178 pagesThe Children's Code Bill, 2022 FinalKaka MwenyaNo ratings yet
- US V RodgersDocument12 pagesUS V RodgersMelissa BoughtonNo ratings yet
- OPPro Psychometric PropertiesDocument3 pagesOPPro Psychometric PropertiesShaniceNo ratings yet
- Tutorial 6Document6 pagesTutorial 6guddu guptaNo ratings yet
- Kel 3 A Midwifery Model of Care ForDocument13 pagesKel 3 A Midwifery Model of Care ForWawa KurniaNo ratings yet
- Artificial Intelligence Technology and Its Relation To Staff Nurses'Document21 pagesArtificial Intelligence Technology and Its Relation To Staff Nurses'shahinazhussein84No ratings yet
- EFFECTS OF ALUGBATI (Basella Alba) On The Growth Performance of Mallard DuckDocument7 pagesEFFECTS OF ALUGBATI (Basella Alba) On The Growth Performance of Mallard DuckCyLo PatricioNo ratings yet
- Isbar WorksheetsDocument2 pagesIsbar Worksheetsapi-688564858No ratings yet
- Mobile CrechesDocument9 pagesMobile CrechesPa Pa PandeyjiNo ratings yet
- Good Morning Class! February 10, 2021: Tle-CarpentryDocument57 pagesGood Morning Class! February 10, 2021: Tle-CarpentryGlenn Fortades SalandananNo ratings yet
- ESSAYDocument1 pageESSAYRachellNo ratings yet
- Research Journal The Pendulum 2018 CompressedDocument144 pagesResearch Journal The Pendulum 2018 Compressedgladys damNo ratings yet
- 2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Document63 pages2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Andy DazNo ratings yet
- Body Mass IndexDocument3 pagesBody Mass IndexJohn Vincent Aguas LptNo ratings yet
- Hbo Midterm Exam Reviewer PDFDocument11 pagesHbo Midterm Exam Reviewer PDFMary Ellen LuceñaNo ratings yet
- FEM 3202-3 LipidDocument15 pagesFEM 3202-3 LipidRon ChongNo ratings yet
- MediCover Graduate StandardDocument28 pagesMediCover Graduate StandardNhung LuuNo ratings yet
- Media, Erotics, and Transnational AsiaDocument389 pagesMedia, Erotics, and Transnational AsiaMaria Fernanda Martinez0% (1)
- EAP Module 8 Concept PaperDocument17 pagesEAP Module 8 Concept PaperJc S. EstaresNo ratings yet
- Tired 2. Motivated 3. Excited 4. Scared 5. Angry 6. Happy 7. Disappointed 8. Bored 9. Delighted 10.sadDocument11 pagesTired 2. Motivated 3. Excited 4. Scared 5. Angry 6. Happy 7. Disappointed 8. Bored 9. Delighted 10.sadAnita Zarza BandaNo ratings yet
- Risk Assessment ExampleDocument3 pagesRisk Assessment Examplecotin006No ratings yet
- Open Stabilization of Acute Acromioclavicular Joint Dislocation Using Twin Tail Tightrope SystemDocument6 pagesOpen Stabilization of Acute Acromioclavicular Joint Dislocation Using Twin Tail Tightrope SystemParaliov TiberiuNo ratings yet