You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Sepsis. The Evolution in Definition, Pathophysiology, and ManagementDocument13 pagesSepsis. The Evolution in Definition, Pathophysiology, and ManagementIvan Tintaya UrureNo ratings yet
- 4 20190629 Detty Cochrane Indonesia UGM Champion Systematic ReviewDocument87 pages4 20190629 Detty Cochrane Indonesia UGM Champion Systematic ReviewRafaela LennyNo ratings yet
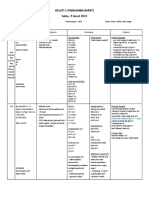
- Operan Jaga 5 Maret 2022Document29 pagesOperan Jaga 5 Maret 2022Rafaela LennyNo ratings yet
- Example: A: "Would You Like To Count The Sum?" B: "OK" A: "Let's Count The Number" B: "OK"Document2 pagesExample: A: "Would You Like To Count The Sum?" B: "OK" A: "Let's Count The Number" B: "OK"Rafaela LennyNo ratings yet
- Picture, Flashcard, Worksheet: Date: September 16 2020 Grade: 1 Lesson: Parts of The FaceDocument2 pagesPicture, Flashcard, Worksheet: Date: September 16 2020 Grade: 1 Lesson: Parts of The FaceRafaela LennyNo ratings yet
- Date: Grade: 3 Lesson: My HobbiesDocument2 pagesDate: Grade: 3 Lesson: My HobbiesRafaela LennyNo ratings yet
- Autoimmune Hemolytic Anemia During Pregnancy With Hemolytic Disease in The NewbornDocument6 pagesAutoimmune Hemolytic Anemia During Pregnancy With Hemolytic Disease in The NewbornRafaela LennyNo ratings yet
- Retinopathy of Prematurity (ROP) : Melissa Andrews BME 281 Sec 2Document7 pagesRetinopathy of Prematurity (ROP) : Melissa Andrews BME 281 Sec 2Rafaela LennyNo ratings yet
- TK03 Gagal Tumbuh Gabungan FinalDocument12 pagesTK03 Gagal Tumbuh Gabungan FinalRafaela LennyNo ratings yet
- Functional Gastrointestinal Disorders History Pathophysiology Clinical Features and Rome IVDocument20 pagesFunctional Gastrointestinal Disorders History Pathophysiology Clinical Features and Rome IVwenyinriantoNo ratings yet
- Assesmen Pasien GeriatriDocument7 pagesAssesmen Pasien GeriatriRafaela LennyNo ratings yet
- Physics Holo - Lab Learning Experience: Using Smartglasses For Augmented Reality Labwork To Foster The Concepts of Heat ConductionDocument14 pagesPhysics Holo - Lab Learning Experience: Using Smartglasses For Augmented Reality Labwork To Foster The Concepts of Heat ConductionRafaela LennyNo ratings yet
- Lect 4 Menziesrctlecture4 Analysisjul2015Document42 pagesLect 4 Menziesrctlecture4 Analysisjul2015Rafaela LennyNo ratings yet
- Retinopathy of Prematurity (ROP) : Melissa Andrews BME 281 Sec 2Document7 pagesRetinopathy of Prematurity (ROP) : Melissa Andrews BME 281 Sec 2Rafaela LennyNo ratings yet
- AUGMENTIN Syrup: What Is in This Leaflet?Document5 pagesAUGMENTIN Syrup: What Is in This Leaflet?Rafaela LennyNo ratings yet
- 3399 On REG Congress CertificateDocument1 page3399 On REG Congress CertificateRafaela LennyNo ratings yet
- DengueDocument67 pagesDengueRafaela LennyNo ratings yet
- The Impact of Duration of Using Superabsorbent Diaper On The Incidence of Urinary Tract Infection in Children 2161 0959.1000180Document5 pagesThe Impact of Duration of Using Superabsorbent Diaper On The Incidence of Urinary Tract Infection in Children 2161 0959.1000180Rafaela LennyNo ratings yet
- Functional Dyspepsia: Future Perspectives in GastroenterologyDocument77 pagesFunctional Dyspepsia: Future Perspectives in GastroenterologyRafaela LennyNo ratings yet
- Functional Dyspepsia: Future Perspectives in GastroenterologyDocument77 pagesFunctional Dyspepsia: Future Perspectives in GastroenterologyRafaela LennyNo ratings yet
- FIGOCEDocument11 pagesFIGOCEAldwin TanuwijayaNo ratings yet
- C.5 Encopresis 0072012Document14 pagesC.5 Encopresis 0072012Indah Afriani Nasution100% (1)
- Functional Dyspepsia: Future Perspectives in GastroenterologyDocument77 pagesFunctional Dyspepsia: Future Perspectives in GastroenterologyRafaela LennyNo ratings yet
- Hunger Rating ScaleDocument1 pageHunger Rating ScaleRafaela LennyNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Strength of Materials: 2. Assume Missing Data, If Any, SuitablyDocument2 pagesStrength of Materials: 2. Assume Missing Data, If Any, SuitablynvnrevNo ratings yet
- Art Lab For Little Kids - Susan Schwake PDFDocument146 pagesArt Lab For Little Kids - Susan Schwake PDFEmma Alfonzo67% (3)
- Accesorios Del Lamborghini VenenoDocument31 pagesAccesorios Del Lamborghini VenenoVicente Gil PalopNo ratings yet
- Latihan Soal Report TextDocument28 pagesLatihan Soal Report TextHidayatul HikmahNo ratings yet
- Gulika in Vedic AstrologyDocument8 pagesGulika in Vedic AstrologyCatchdgreen100% (1)
- Aljac Sampler: Environmentally Acceptable, Operationally Efficient and Safe, Eliminating Any Product LossDocument3 pagesAljac Sampler: Environmentally Acceptable, Operationally Efficient and Safe, Eliminating Any Product LossT. LimNo ratings yet
- Yu-Gi-Oh GX Duel Academy - Written ExamDocument26 pagesYu-Gi-Oh GX Duel Academy - Written ExamisishamalielNo ratings yet
- ASD Fan CalculatorsDocument14 pagesASD Fan CalculatorslubricacionNo ratings yet
- Looking For Cochlear Dead Regions A Clinical Experience With TEN TestDocument9 pagesLooking For Cochlear Dead Regions A Clinical Experience With TEN TestVinay S NNo ratings yet
- BNB SB0114Document4 pagesBNB SB0114graziana100% (2)
- Annals of The New York Academy of Sciences - 2023 - Hess - Accelerating Action To Reduce Anemia Review of Causes and RiskDocument13 pagesAnnals of The New York Academy of Sciences - 2023 - Hess - Accelerating Action To Reduce Anemia Review of Causes and RiskIdmNo ratings yet
- AdsfatreewerwertgdsfDocument1 pageAdsfatreewerwertgdsfJhonel AguilarNo ratings yet
- TP260SR Tier 3 TC002-1037Document1 pageTP260SR Tier 3 TC002-1037Jorge GalarceNo ratings yet
- bNSG9000 Datasheet 2Document3 pagesbNSG9000 Datasheet 2RobertNo ratings yet
- Philippine Airlines Reservation New Timings Dep - 230314 - 193643Document7 pagesPhilippine Airlines Reservation New Timings Dep - 230314 - 193643sophia buiserNo ratings yet
- Vertical HabitatDocument6 pagesVertical HabitatAbdul SakurNo ratings yet
- People at Virology: Dmitri Iosifovich Ivanovsky - Founders of VirologyDocument2 pagesPeople at Virology: Dmitri Iosifovich Ivanovsky - Founders of VirologyFae BladeNo ratings yet
- J. Agric. Food Chem. 2005, 53, 9010-9016Document8 pagesJ. Agric. Food Chem. 2005, 53, 9010-9016Jatyr OliveiraNo ratings yet
- Easy Guide For Fujitsu T901 LaptopDocument141 pagesEasy Guide For Fujitsu T901 LaptopElaineNo ratings yet
- Basic Resistance Training GP5Document20 pagesBasic Resistance Training GP5matt.tubieron23No ratings yet
- ASI Hammer Injection Block ManualDocument16 pagesASI Hammer Injection Block ManualGerardo Manuel FloresNo ratings yet
- Economics 526 - Mathematics For Economists: Day(s) Time LocationDocument5 pagesEconomics 526 - Mathematics For Economists: Day(s) Time LocationGaurav JakhuNo ratings yet
- Igcse ReadingDocument4 pagesIgcse ReadingIvonne PuspakencanaNo ratings yet
- Bushing TestingDocument8 pagesBushing TestingjoseNo ratings yet
- Astro 429 Assignment 2 AlbertaDocument2 pagesAstro 429 Assignment 2 AlbertatarakNo ratings yet
- Architect As An Environmental PlannerDocument14 pagesArchitect As An Environmental PlannerJames Adrian MoralNo ratings yet
- Fate NumeneraDocument24 pagesFate Numeneraimaginaari100% (1)
- Dobdsm 304Document39 pagesDobdsm 304LuisangelDueñasNo ratings yet
- Unit II Construction PracticesDocument61 pagesUnit II Construction PracticesiploguNo ratings yet
- CPHL 214 Assignment 6Document2 pagesCPHL 214 Assignment 6NazNo ratings yet