You might also like
- QuietDocument3 pagesQuietPatrick McClair33% (3)
- Abnormal Psychology Study GuideDocument243 pagesAbnormal Psychology Study GuideAllissa Michelle Kimker83% (23)
- Neurocognitive DisordersDocument31 pagesNeurocognitive DisordersMonina JonesNo ratings yet
- AntipsychoticsDocument58 pagesAntipsychoticsnithin shenoiNo ratings yet
- Antipsychotics Bipolar Disorders OCDDocument78 pagesAntipsychotics Bipolar Disorders OCDCharles YiuNo ratings yet
- Annie Audition PackDocument17 pagesAnnie Audition PackPatrick McClair100% (3)
- Away in A MangerDocument1 pageAway in A MangerPatrick McClairNo ratings yet
- Leonard Bernstein - An American Musician by Allen Shawn (DR - Soc)Document359 pagesLeonard Bernstein - An American Musician by Allen Shawn (DR - Soc)Axel Juárez100% (4)
- AntipsychoticsDocument47 pagesAntipsychoticsammar_ahmed_19No ratings yet
- Lecture No. 5 Organic Mental Disorders in PsychiatryDocument41 pagesLecture No. 5 Organic Mental Disorders in Psychiatryozgur.yonlukNo ratings yet
- Antipsychotic Drugs: (Neuroleptics, Major Tranquillizer Ataractic)Document63 pagesAntipsychotic Drugs: (Neuroleptics, Major Tranquillizer Ataractic)Muhammad Masoom Akhtar100% (1)
- AntidepresentDocument34 pagesAntidepresentmariaNo ratings yet
- Organic Brain SyndromeDocument40 pagesOrganic Brain SyndromeShaz ZrinNo ratings yet
- AlzheimerDocument16 pagesAlzheimerjudii01No ratings yet
- PIL Cases (Midterms)Document231 pagesPIL Cases (Midterms)Yulo Vincent Bucayu PanuncioNo ratings yet
- Unit 2 Abnormal PsychologyDocument44 pagesUnit 2 Abnormal PsychologyMohammed SaniNo ratings yet
- Annie Male Audition PackDocument25 pagesAnnie Male Audition PackPatrick McClairNo ratings yet
- Analysis Rizal's RetractionDocument20 pagesAnalysis Rizal's RetractionGuki SuzukiNo ratings yet
- Chapter 2 Conceptualizing Abnormal Psychology PDFDocument67 pagesChapter 2 Conceptualizing Abnormal Psychology PDFGabriel Jeremy Ortega100% (1)
- Delirium and Its ManagmentDocument64 pagesDelirium and Its ManagmentViren Solanki100% (1)
- Neurocognitive DisordersDocument26 pagesNeurocognitive DisordersGede GiriNo ratings yet
- Etiology of PsychopathologyDocument61 pagesEtiology of PsychopathologyAdrishya100% (4)
- SchizophreniaDocument55 pagesSchizophreniasoran muzeyinNo ratings yet
- Business Ethics NotesDocument65 pagesBusiness Ethics NotesRahul M. DasNo ratings yet
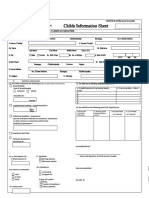
- I. Identifying Information NOTE Fields ( ) Asterisk Are Required Fields 1Document3 pagesI. Identifying Information NOTE Fields ( ) Asterisk Are Required Fields 1adoptify89% (28)
- Neurobiology of SchizophreniaDocument54 pagesNeurobiology of SchizophreniaPriyash JainNo ratings yet
- Introduction IFRS17Document9 pagesIntroduction IFRS17Ruben Perez Espinoza100% (1)
- DementiaDocument40 pagesDementiakhusnulNo ratings yet
- Li Meixiu (Ellen) : JMS UniversityDocument46 pagesLi Meixiu (Ellen) : JMS UniversityMunir AhmedNo ratings yet
- ANXIETY Disorders Final YearDocument52 pagesANXIETY Disorders Final YearMuhammad MakkiNo ratings yet
- Alterations in Cognitive Systems, Cerebral Hemodynamics, and Motor FunctionDocument54 pagesAlterations in Cognitive Systems, Cerebral Hemodynamics, and Motor FunctionKeatonNo ratings yet
- Delirium ADocument69 pagesDelirium AAbelNo ratings yet
- Cliffnotes For NBME (Slides)Document11 pagesCliffnotes For NBME (Slides)Cassandra BNo ratings yet
- EON - 2020 - Mentall Illness - ES - 1pageDocument40 pagesEON - 2020 - Mentall Illness - ES - 1pageJAMESNo ratings yet
- Drug Therapy of Psychosis and Mania and Bipolar Disorders Igor IezhitsaDocument37 pagesDrug Therapy of Psychosis and Mania and Bipolar Disorders Igor IezhitsaZobayer AhmedNo ratings yet
- Group ThreeDocument45 pagesGroup ThreeAYO NELSONNo ratings yet
- The Elderly BrainDocument18 pagesThe Elderly BrainferronocampoNo ratings yet
- Psych 160 Chapter 18Document9 pagesPsych 160 Chapter 18Rashia LubuguinNo ratings yet
- 4 AntipsychoticDocument109 pages4 AntipsychoticMtw Wond100% (1)
- Slides SchizophreniaDocument28 pagesSlides SchizophreniaEesha TahirNo ratings yet
- Neurobiology of Schizophrenia (Part 1)Document92 pagesNeurobiology of Schizophrenia (Part 1)Sid KolgeNo ratings yet
- Pharma - Anti Parkinsons Dra JusayanDocument105 pagesPharma - Anti Parkinsons Dra JusayanNikko AgcaoiliNo ratings yet
- PBL 2Document16 pagesPBL 2alreemNo ratings yet
- Unit 3 Nervous SystemDocument58 pagesUnit 3 Nervous SystemdhanashriNo ratings yet
- Schizophrenia and Assotiated DisordersDocument59 pagesSchizophrenia and Assotiated DisordersJessel Mae JavierNo ratings yet
- Dementia AdDocument40 pagesDementia Adknowledgeguruos179No ratings yet
- Pemicu 3 Blok Saraf: Jessica Gracia 405140041Document137 pagesPemicu 3 Blok Saraf: Jessica Gracia 405140041Jessica GraciaNo ratings yet
- Kasus Alzeimer Pada AnakDocument13 pagesKasus Alzeimer Pada AnakAbqariyahNo ratings yet
- Schizophrenia and Other Psychotic Disorders: Southern Philippines Medical CenterDocument44 pagesSchizophrenia and Other Psychotic Disorders: Southern Philippines Medical CenterMaureen JadeNo ratings yet
- DementiaDocument74 pagesDementiaAndika ResaNo ratings yet
- Psychiatry Nakal 2Document13 pagesPsychiatry Nakal 2drutkarsh vashishthaNo ratings yet
- Organic Mental DisorderDocument40 pagesOrganic Mental DisorderSumam NeveenNo ratings yet
- Psychiatry 104Document55 pagesPsychiatry 104Vaso TalakvadzeNo ratings yet
- Schizophrenia Part 2Document18 pagesSchizophrenia Part 2MUHD SUHAILNo ratings yet
- Confusion: Koech KM Fri Feb 12, 2010Document23 pagesConfusion: Koech KM Fri Feb 12, 2010api-50425236No ratings yet
- Alzheimer's Disease: Causes, Effects, and TreatmentsDocument14 pagesAlzheimer's Disease: Causes, Effects, and TreatmentsGundappa RaoNo ratings yet
- 9.mental Disorders Due To A General Medical Condition and Organic Brain Damages PDFDocument50 pages9.mental Disorders Due To A General Medical Condition and Organic Brain Damages PDFchairihidayatzaNo ratings yet
- 9.mental Disorders Due To A General Medical Condition and Organic Brain Damages.Document50 pages9.mental Disorders Due To A General Medical Condition and Organic Brain Damages.chairihidayatzaNo ratings yet
- Alzheimers Disease and Chediak Hijashi SyndromeDocument47 pagesAlzheimers Disease and Chediak Hijashi Syndromecarmelo aguirreNo ratings yet
- Anxiety DisorderDocument42 pagesAnxiety Disorderfemfen1225100% (3)
- SchizophreniaDocument20 pagesSchizophreniaNabeel RayedNo ratings yet
- Slides Mood DisordersDocument15 pagesSlides Mood DisordersEesha TahirNo ratings yet
- Alzheimer's DiseaseDocument61 pagesAlzheimer's DiseaseilalcNo ratings yet
- Parkinson's DiseaseDocument37 pagesParkinson's DiseaseAhmed OsamaNo ratings yet
- Antipsychotics 2020Document39 pagesAntipsychotics 2020ciaranNo ratings yet
- DEMENTIA: Alzheimer's Disease and Vascular Dementia: Christian Kamallan NeurologistDocument86 pagesDEMENTIA: Alzheimer's Disease and Vascular Dementia: Christian Kamallan NeurologistLuthfi HakimNo ratings yet
- 1-2 Concepts of NormalityDocument8 pages1-2 Concepts of NormalitynesumaNo ratings yet
- Neurological Disorders: Paul Kelner, M.DDocument97 pagesNeurological Disorders: Paul Kelner, M.DDrGasnasNo ratings yet
- Alege CorectDocument41 pagesAlege CorectIna RomaniucNo ratings yet
- Mental Health - Chapter 10Document4 pagesMental Health - Chapter 10McKinley Anne CarlisleNo ratings yet
- Psychopharmacology: A Clinician's Guide for the Effective use of Psychotropic MedicationsFrom EverandPsychopharmacology: A Clinician's Guide for the Effective use of Psychotropic MedicationsNo ratings yet
- Airdrie Town Hall Tech SpecDocument5 pagesAirdrie Town Hall Tech SpecPatrick McClairNo ratings yet
- 1y4u4i4o4p4 (4) 4/4a 1yip) A 15p5y5a5i5) 5y5p5i5a5) 5p 1uo (/ 16u5 (5/5o5u5/5 (5o5u5 (5Document1 page1y4u4i4o4p4 (4) 4/4a 1yip) A 15p5y5a5i5) 5y5p5i5a5) 5p 1uo (/ 16u5 (5/5o5u5/5 (5o5u5 (5Patrick McClairNo ratings yet
- Grade 4 Piano 2021/22: ScalesDocument2 pagesGrade 4 Piano 2021/22: ScalesPatrick McClairNo ratings yet
- Grade 2 Piano 2021/22: NameDocument2 pagesGrade 2 Piano 2021/22: NamePatrick McClairNo ratings yet
- Lecture 3 - Mental Health Pharmacy - StigmaDocument12 pagesLecture 3 - Mental Health Pharmacy - StigmaPatrick McClairNo ratings yet
- Medicines Information Scenario 1Document2 pagesMedicines Information Scenario 1Patrick McClair100% (1)
- Grade 1 Piano 2021/22: NameDocument2 pagesGrade 1 Piano 2021/22: NamePatrick McClairNo ratings yet
- Lecture 6 - AnxietyDocument32 pagesLecture 6 - AnxietyPatrick McClairNo ratings yet
- Old BiblioDocument1 pageOld BiblioPatrick McClairNo ratings yet
- ABRSM 2017 18 Piano Pieces Gr1 PDFDocument12 pagesABRSM 2017 18 Piano Pieces Gr1 PDFPatrick McClairNo ratings yet
- Brass LessonsDocument1 pageBrass LessonsPatrick McClairNo ratings yet
- Tuesdays Thursdays Sundays Notes: Tuesday 18 June Thursday 20 JuneDocument1 pageTuesdays Thursdays Sundays Notes: Tuesday 18 June Thursday 20 JunePatrick McClairNo ratings yet
- Atkins DietDocument1 pageAtkins DietPatrick McClairNo ratings yet
- Emma NotesDocument2 pagesEmma NotesPatrick McClairNo ratings yet
- A-Side Soul Set ListDocument2 pagesA-Side Soul Set ListPatrick McClairNo ratings yet
- Good Online Quizzes and Mnemonics HintDocument1 pageGood Online Quizzes and Mnemonics HintPatrick McClairNo ratings yet
- Stage CuesDocument2 pagesStage CuesPatrick McClairNo ratings yet
- TRR3404442 ChecklistDocument10 pagesTRR3404442 ChecklistChishanu KaromboNo ratings yet
- Modeling Tuned Mass Dampers (TMD) in Autodesk Robot Structural Analysis Professional Description of ExampleDocument1 pageModeling Tuned Mass Dampers (TMD) in Autodesk Robot Structural Analysis Professional Description of ExampleJillian Howard0% (1)
- Jealousy in Othello PDFDocument6 pagesJealousy in Othello PDFjunaidyousaf50% (2)
- Servicewide Specialists vs. CaDocument9 pagesServicewide Specialists vs. CaJohn FerarenNo ratings yet
- Fyudsp PDFDocument115 pagesFyudsp PDFninaNo ratings yet
- Richard WurmbrandDocument7 pagesRichard WurmbrandMelvin ShajiNo ratings yet
- Reflection Paper - Lost in TranslationDocument1 pageReflection Paper - Lost in TranslationBhavesh D JainNo ratings yet
- Minitab PDFDocument83 pagesMinitab PDFHalimi Abdellah TakieddineNo ratings yet
- Study of Consumer Buying Behaviour in Reliance FreshDocument80 pagesStudy of Consumer Buying Behaviour in Reliance Freshamit@8386% (14)
- HRM RDocument8 pagesHRM RNAVU PUBGNo ratings yet
- 8 Case Study and Grounded TheoryDocument51 pages8 Case Study and Grounded TheoryAC BalioNo ratings yet
- Formal Biology Lab ReportsDocument2 pagesFormal Biology Lab ReportsSweetie AndersonNo ratings yet
- Understand The SelfDocument4 pagesUnderstand The SelfJanna Marie DeocampoNo ratings yet
- Insurance TextbookDocument131 pagesInsurance TextbookbookboomingNo ratings yet
- Chapter Iii - Research Methodology - Measures of Central Tendency-1Document5 pagesChapter Iii - Research Methodology - Measures of Central Tendency-1Hermie Rose AlvarezNo ratings yet
- SSCBS - FDPDocument7 pagesSSCBS - FDPkunalNo ratings yet
- COOKERY9-Q1-WEEK3Document3 pagesCOOKERY9-Q1-WEEK3Merlinda PacquiaoNo ratings yet
- Chap 02 (Fluid Mechanic) PDFDocument65 pagesChap 02 (Fluid Mechanic) PDFK'roll Azham AvearNo ratings yet
- Lab 1 Compile SBFDocument15 pagesLab 1 Compile SBFAin SufizaNo ratings yet
- HEYM - Al Razi and AlchemyDocument9 pagesHEYM - Al Razi and AlchemyjesusegidoNo ratings yet
- Kecskemét College Kecskemét CollegeDocument9 pagesKecskemét College Kecskemét CollegeBeatrix KovácsNo ratings yet
- David Walliams Writing Childrens Books V1Document64 pagesDavid Walliams Writing Childrens Books V1Tatjana KeninaNo ratings yet
- Cinderella (Text + Audio)Document16 pagesCinderella (Text + Audio)Anna AbashviliNo ratings yet