You might also like
- Drugs Acting On The Respiratory System: Wednesday, 9 March 2022 3:47 AmDocument6 pagesDrugs Acting On The Respiratory System: Wednesday, 9 March 2022 3:47 AmAdiel CalsaNo ratings yet
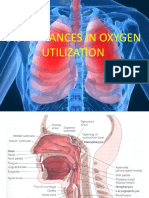
- Slides. Disturbances in Oxygen Utilization 2 1Document101 pagesSlides. Disturbances in Oxygen Utilization 2 1SHARMAINE ANNE POLICIOSNo ratings yet
- Drugs URS IntroDocument4 pagesDrugs URS IntroAdiel CalsaNo ratings yet
- Respiratory DrugsDocument140 pagesRespiratory Drugsmoncalshareen3No ratings yet
- Drugs Affecting The Respiratory System PPPDocument35 pagesDrugs Affecting The Respiratory System PPPChristopher VelonzaNo ratings yet
- Pharmacology: Drugs Acting On The Respiratory SystemDocument7 pagesPharmacology: Drugs Acting On The Respiratory SystemShun Reigh SumilangNo ratings yet
- Drugs Affecting the Respiratory SystemDocument137 pagesDrugs Affecting the Respiratory SystemUmar Bakshi100% (1)
- Asthma Nur220 Student PowerpointDocument26 pagesAsthma Nur220 Student PowerpointPaula BissetteNo ratings yet
- Ikhlas Muhammad Jenie Physiology Department: Fkik UmyDocument56 pagesIkhlas Muhammad Jenie Physiology Department: Fkik Umyade ayuningsih utamiNo ratings yet
- Respiratory AgentsDocument65 pagesRespiratory AgentsChelsea Mariette AndradeNo ratings yet
- Bronchial Asthma Power PointDocument44 pagesBronchial Asthma Power Pointjohnbech07No ratings yet
- Group 3 Respiratory SystemDocument69 pagesGroup 3 Respiratory Systemgoodemonz15No ratings yet
- Respiratory SystemDocument104 pagesRespiratory SystemKatisha JosephNo ratings yet
- Drugs Affecting The Respiratory SystemDocument75 pagesDrugs Affecting The Respiratory Systemone_nd_onlyuNo ratings yet
- Urti Lrti Drugs 2023Document8 pagesUrti Lrti Drugs 2023dlabdon0310No ratings yet
- Asthama & COPDDocument84 pagesAsthama & COPDAbdullah BhattiNo ratings yet
- Drugs Affecting the Respiratory SystemDocument112 pagesDrugs Affecting the Respiratory SystemRizky LestariNo ratings yet
- Understanding the Phases, Types and Treatment of CoughDocument58 pagesUnderstanding the Phases, Types and Treatment of CoughRaghu NadhNo ratings yet
- Drugs Affecting Respiratory SystemDocument65 pagesDrugs Affecting Respiratory SystemvivianNo ratings yet
- Drugs Affecting The Respiratory Systems: Kuntarti, SKP, MbiomedDocument32 pagesDrugs Affecting The Respiratory Systems: Kuntarti, SKP, MbiomedRichard BungaNo ratings yet
- Respiratory SystemDocument19 pagesRespiratory SystemOctavia. GNo ratings yet
- Respiratory System Herbs GuideDocument43 pagesRespiratory System Herbs GuideDylan StaakNo ratings yet
- Dr. Swagath, HassanDocument29 pagesDr. Swagath, HassanSwagath NNo ratings yet
- Asthma SIM AnswersDocument4 pagesAsthma SIM Answersscorpioaj133No ratings yet
- Lecture 14 - Pharmacology of Drugs Used in Bronchial Asthma L0 COPD - EditedDocument42 pagesLecture 14 - Pharmacology of Drugs Used in Bronchial Asthma L0 COPD - EditedAbdallah AlasalNo ratings yet
- Pharma Midterm ReviewerDocument45 pagesPharma Midterm ReviewerCarlos Miguel AndalNo ratings yet
- MCN CompiledDocument71 pagesMCN CompiledJœnríčk AzueloNo ratings yet
- File 18585Document15 pagesFile 18585Mohammed MuthanaNo ratings yet
- CHD AsthmaDocument20 pagesCHD AsthmaRj MagpayoNo ratings yet
- Case StudyDocument7 pagesCase StudyjoviloumNo ratings yet
- 5 - Respiratory AssessmentDocument61 pages5 - Respiratory AssessmentAbboud Ali100% (1)
- Pharmacology Gas ExchangeDocument2 pagesPharmacology Gas ExchangekatrinasdNo ratings yet
- Week 2 - Drugs Used in Asthma: Tinatin JomidavaDocument59 pagesWeek 2 - Drugs Used in Asthma: Tinatin JomidavaTiko JomidavaNo ratings yet
- Cough, Cold and Flu TreatmentDocument7 pagesCough, Cold and Flu TreatmentAbdul MajeedNo ratings yet
- Antiasthamatic DrugsDocument72 pagesAntiasthamatic DrugsDeepak kumarNo ratings yet
- 2cough and ExpectationDocument37 pages2cough and ExpectationMar ClrNo ratings yet
- Case Study of AsthmaDocument6 pagesCase Study of Asthmabuzz Q100% (4)
- Respiratory EMDocument51 pagesRespiratory EMMwalimu Hachalu FayeNo ratings yet
- ASTHMADocument16 pagesASTHMANavneet GillNo ratings yet
- DRUG TREATMENT OF BRONCHIAL ASTHMADocument39 pagesDRUG TREATMENT OF BRONCHIAL ASTHMAHomeground entertainmentNo ratings yet
- MS RESPIbfrDocument13 pagesMS RESPIbfrEmeroot RootNo ratings yet
- Day 15 - NCM-109 Children With Alteration in Oxygenation (A)Document50 pagesDay 15 - NCM-109 Children With Alteration in Oxygenation (A)Sheena Patricia ArasulaNo ratings yet
- Acute Respiratory Failure: Causes, Signs, TreatmentDocument6 pagesAcute Respiratory Failure: Causes, Signs, Treatmentniki estuNo ratings yet
- Bronchial Asthma Types Treatments ComplicationsDocument12 pagesBronchial Asthma Types Treatments ComplicationsRAMNo ratings yet
- Drugs Affecting Respiratory SystemDocument62 pagesDrugs Affecting Respiratory Systemyunita ekawatiNo ratings yet
- Asthma Diagnosis and Treatment OverviewDocument82 pagesAsthma Diagnosis and Treatment OverviewImmanuel100% (1)
- Asthma: A Guide to Its Definition, Types, Causes, Symptoms and TreatmentDocument16 pagesAsthma: A Guide to Its Definition, Types, Causes, Symptoms and TreatmentJuma SammyNo ratings yet
- Asthma Drugs GuideDocument135 pagesAsthma Drugs GuideDR. MUSICNo ratings yet
- Bronchodilators and Other Respiratory DrugsDocument44 pagesBronchodilators and Other Respiratory DrugsastriedamaliaamanatNo ratings yet
- NCM 106 FinalsDocument55 pagesNCM 106 FinalsKyle BagacNo ratings yet
- 4.control of VentilationDocument40 pages4.control of VentilationEbin EbenezerNo ratings yet
- k12, Pa, Pathology of Copd - rts1-k12Document46 pagesk12, Pa, Pathology of Copd - rts1-k12ashtridNo ratings yet
- (Respi) Lo Week 2 Tutorial 1Document10 pages(Respi) Lo Week 2 Tutorial 1KintanNo ratings yet
- Bronchial AsthmaDocument95 pagesBronchial AsthmaBrian BrownNo ratings yet
- ASTHMADocument4 pagesASTHMAKhasim AgwilangNo ratings yet
- Drugs For Cough: DR - Vijay BhushanamDocument14 pagesDrugs For Cough: DR - Vijay Bhushanamheka_amrongNo ratings yet
- Bronchial AsthmaDocument54 pagesBronchial AsthmaSehar162100% (2)
- Chapter 4 HTDocument52 pagesChapter 4 HTtesfamichael mengistuNo ratings yet
- Anaphylaxis: A Practical GuideFrom EverandAnaphylaxis: A Practical GuideAnne K. EllisNo ratings yet
- Homeopathic Remedy Pictures Vicki Mathison Frans Kusse.11789 - 1 PDFDocument19 pagesHomeopathic Remedy Pictures Vicki Mathison Frans Kusse.11789 - 1 PDFPrasanta ChatterjeeNo ratings yet
- Top Notch 3 2ND Edition Workbook Answer Key PDFDocument16 pagesTop Notch 3 2ND Edition Workbook Answer Key PDFMaycol Antonio Rojas100% (3)
- WHO IMAI Acute - Care PDFDocument138 pagesWHO IMAI Acute - Care PDFJohn Philip TiongcoNo ratings yet
- Ineffective Airway ClearanceDocument6 pagesIneffective Airway Clearanceapi-252726911No ratings yet
- NCMB 312 Lec Course Task CU3Document2 pagesNCMB 312 Lec Course Task CU3Mushy_ayaNo ratings yet
- EXAM 3 20210405 C11 NUR310G.C Health Assessment PDFDocument37 pagesEXAM 3 20210405 C11 NUR310G.C Health Assessment PDFCeciliaNo ratings yet
- Sample Collection Roleplay Shows Sputum Test ProcessDocument3 pagesSample Collection Roleplay Shows Sputum Test ProcessPutu RikaNo ratings yet
- Lagundi Tea For Stronger Lungs and LiverDocument2 pagesLagundi Tea For Stronger Lungs and LiverJohn Mark LedesmaNo ratings yet
- Asthma Nursing Care Management and Study GuideDocument7 pagesAsthma Nursing Care Management and Study GuideRamakrishna BadeNo ratings yet
- Occupational Health Risks Among The WorkersDocument4 pagesOccupational Health Risks Among The WorkersVijay PrajapatiNo ratings yet
- Drugs For Cough: Pharyngeal DemulcentsDocument5 pagesDrugs For Cough: Pharyngeal DemulcentsArpan Guchhait100% (1)
- Allens KeynotesDocument145 pagesAllens KeynotesParas ManglaNo ratings yet
- GINA 2017 Teaching Slide Set FullDocument17 pagesGINA 2017 Teaching Slide Set FullLorenzoVasquezDatul100% (3)
- BronchitisDocument4 pagesBronchitisGokul SmartNo ratings yet
- Medicinal PlantsDocument34 pagesMedicinal PlantsmathewNo ratings yet
- COMSEP ProblemSetDocument29 pagesCOMSEP ProblemSettasha2gNo ratings yet
- What is COPD? Understanding Chronic Obstructive Pulmonary DiseaseDocument9 pagesWhat is COPD? Understanding Chronic Obstructive Pulmonary Diseasemartha kurniaNo ratings yet
- Baiae NCPDocument1 pageBaiae NCPreignyfayeNo ratings yet
- Pneumonia Is A Condition That Causes The Lungs To Become Inflamed As A Result of A BacterialDocument3 pagesPneumonia Is A Condition That Causes The Lungs To Become Inflamed As A Result of A BacterialDhonnalyn Amene CaballeroNo ratings yet
- CAWAYAN ES ConPlan For COVID 19 ResurgencesDocument34 pagesCAWAYAN ES ConPlan For COVID 19 ResurgencesCAWAYAN ELEMENTARY SCHOOLNo ratings yet
- Kali MuriaticumDocument7 pagesKali MuriaticumkiradoooNo ratings yet
- Sarabjit SeminarDocument290 pagesSarabjit SeminarparmeshoriNo ratings yet
- Anatomic Therapy Guide to Healing DiseasesDocument364 pagesAnatomic Therapy Guide to Healing Diseasesrahul_choubey_9No ratings yet
- Lung ExaminationDocument14 pagesLung Examinationსალომე მუმლაძე “Slay” TMANo ratings yet
- Seafarer's Death Due to Occupational IllnessDocument7 pagesSeafarer's Death Due to Occupational IllnessBenjie PangosfianNo ratings yet
- 872 Short Advanced Reading Comprehension Test 29 With Mcqs and AnswersDocument8 pages872 Short Advanced Reading Comprehension Test 29 With Mcqs and AnswersSaja LolwaNo ratings yet
- Fly Ash - Bottom Ash: Safety Data SheetDocument5 pagesFly Ash - Bottom Ash: Safety Data SheetMatt LNo ratings yet
- ArticleDocument17 pagesArticleRonnie DalgoNo ratings yet
- Submitted To:-Dr. A.P. Singh: Compiled By: - Nisha SharmaDocument8 pagesSubmitted To:-Dr. A.P. Singh: Compiled By: - Nisha SharmaKamal K SharmaNo ratings yet
- Varicocele HealingDocument42 pagesVaricocele Healingrian4me100% (6)