You might also like
- Mumps: Laboratory of Microbiology Faculty of Medicine Brawijaya UniversityDocument69 pagesMumps: Laboratory of Microbiology Faculty of Medicine Brawijaya UniversityKharisulNo ratings yet
- Diseases of Salivary Glands: Prepared By: Dr. Ahlam A. AlesayiDocument96 pagesDiseases of Salivary Glands: Prepared By: Dr. Ahlam A. AlesayiWaqas Iqbal100% (1)
- Otologic Manifestation of Systemic DiseaseDocument57 pagesOtologic Manifestation of Systemic DiseaseHERIZALNo ratings yet
- Enterovirus: Regati Meenakshi ROLL: B30Document27 pagesEnterovirus: Regati Meenakshi ROLL: B30Meena RajNo ratings yet
- Prof. Dalia M. Mohsen Lecture VirologyDocument24 pagesProf. Dalia M. Mohsen Lecture VirologyDalia M. MohsenNo ratings yet
- CYRUSSDocument13 pagesCYRUSSRienna Marie HentoloroNo ratings yet
- Mumps ParotitisDocument28 pagesMumps ParotitisShari' Si WahyuNo ratings yet
- Foot and Mouth DiseasesDocument9 pagesFoot and Mouth Diseaseseutamène ramziNo ratings yet
- 3 Micro 9 - Rna II - Dr. SengsonDocument14 pages3 Micro 9 - Rna II - Dr. SengsonyayayanizaNo ratings yet
- Zoonotic VirusesDocument12 pagesZoonotic VirusesSamuel Ojonugwa AuduNo ratings yet
- Understanding AIDS and RotavirusDocument34 pagesUnderstanding AIDS and RotavirusCrystal Ann TadiamonNo ratings yet
- Sexually Transmitted Infections 19-21Document4 pagesSexually Transmitted Infections 19-21Ashar AhmadNo ratings yet
- Mumps, Measles, Rubella (MMR) 06-07Document31 pagesMumps, Measles, Rubella (MMR) 06-07api-3699361100% (3)
- Exanthems in Infectious DiseasesDocument40 pagesExanthems in Infectious DiseasesHaymond PrasadNo ratings yet
- Mumps (Parotitis)Document28 pagesMumps (Parotitis)SipkhotunWindayaniNo ratings yet
- Common Childhood Infections For CIDocument89 pagesCommon Childhood Infections For CIBeamlak Getachew WoldeselassieNo ratings yet
- 2019 DR - Sgiti WIdyatmoko, SP - PD Mumps (Parotitis)Document37 pages2019 DR - Sgiti WIdyatmoko, SP - PD Mumps (Parotitis)Wahyu FajarNo ratings yet
- Viral Skin RashesDocument26 pagesViral Skin RashesGeoffreyNo ratings yet
- Common Cold: Milan Karki 4062Document20 pagesCommon Cold: Milan Karki 4062BinayaNo ratings yet
- A Guide To Salivary Gland DisordersDocument5 pagesA Guide To Salivary Gland Disordersdanny17phNo ratings yet
- Virus PDFDocument60 pagesVirus PDFrenz bartolomeNo ratings yet
- Infectious DiseasesDocument48 pagesInfectious Diseasesxxxjuanxxx lol its maxNo ratings yet
- ParamyxoviridaeDocument27 pagesParamyxoviridaeFarrah BenoitNo ratings yet
- Lepto Dan RabiesDocument69 pagesLepto Dan RabiesHiszom AsyhariNo ratings yet
- Microbial Diseases of The Nervous SystemDocument18 pagesMicrobial Diseases of The Nervous SystemInah PagariganNo ratings yet
- Common Viral Infections CC Sarmiento DIdacticsDocument87 pagesCommon Viral Infections CC Sarmiento DIdacticsUthuriel27No ratings yet
- REFERAT - Meassles - FirdaDocument19 pagesREFERAT - Meassles - FirdaEriza LuthfansyahNo ratings yet
- 3_VIRUS_29OCT2021Document59 pages3_VIRUS_29OCT2021haiqalfariq07No ratings yet
- Enterovirus: Virologi Klinik KDM 726 Pembimbing: Dr. Abu Rohiman, MS, SPMK (K)Document12 pagesEnterovirus: Virologi Klinik KDM 726 Pembimbing: Dr. Abu Rohiman, MS, SPMK (K)Daniel EdbertNo ratings yet
- Mumps (Parotitis)Document28 pagesMumps (Parotitis)Muna Fiah100% (1)
- Microbiology (Midterms)Document37 pagesMicrobiology (Midterms)Veloria AbegailNo ratings yet
- ParamyxovirusesDocument36 pagesParamyxovirusesRandy BerryNo ratings yet
- Penyakit Virus: - Virus Dna Rna - Virus DNADocument23 pagesPenyakit Virus: - Virus Dna Rna - Virus DNAKelas BNo ratings yet
- Rhinovirus: Otitis Media and Sinusitis. ExacerbationsDocument34 pagesRhinovirus: Otitis Media and Sinusitis. ExacerbationsManisanthosh KumarNo ratings yet
- LDLSKNDDocument46 pagesLDLSKNDFarizka Dwinda HidayatNo ratings yet
- Microbiology PinkDocument3 pagesMicrobiology PinkBenjamin GaliaNo ratings yet
- Lec8 Infectious DiseasesDocument32 pagesLec8 Infectious DiseasesmanuelNo ratings yet
- Picornaviruses: Linus PaulDocument63 pagesPicornaviruses: Linus PaulBrother GeorgeNo ratings yet
- 2022 Intensive Course. MM - Viral Hepatitis & HIV - AP Datin DR Noor ZettiDocument65 pages2022 Intensive Course. MM - Viral Hepatitis & HIV - AP Datin DR Noor ZettiRaja RuzannaNo ratings yet
- Sexually Transmitted DiseasesDocument132 pagesSexually Transmitted DiseasesanitacharisNo ratings yet
- P 1 InfectiousDocument73 pagesP 1 InfectiousHIMANSHU GUPTANo ratings yet
- Infectious OralsDocument164 pagesInfectious OralsHIMANSHU GUPTANo ratings yet
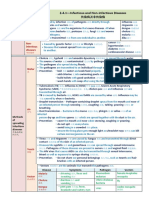
- 2.4.1-Infectious and Non-Infectious DiseasesDocument2 pages2.4.1-Infectious and Non-Infectious DiseasesCHIA YIN MEINo ratings yet
- 5 Nervous Urinary ReproductiveDocument48 pages5 Nervous Urinary Reproductiveesther samonteNo ratings yet
- Human Health and DiseaseDocument6 pagesHuman Health and DiseaseSunil GargNo ratings yet
- Medical Virology: DNA Viruses and HerpesviridaeDocument32 pagesMedical Virology: DNA Viruses and HerpesviridaeTofikNo ratings yet
- Mumps (Parotitis)Document23 pagesMumps (Parotitis)Rahmatullah AhmadNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- PicornaViruses - Medical VirologyDocument32 pagesPicornaViruses - Medical VirologyFarhang ShapouranNo ratings yet
- Epi#3Document19 pagesEpi#3JNo ratings yet
- UnknownDocument87 pagesUnknownKhaled JmalNo ratings yet
- Communicable DiseaseDocument32 pagesCommunicable Diseasekimberly shayneNo ratings yet
- Mikrobiologi VirusDocument29 pagesMikrobiologi VirusNor HashinaNo ratings yet
- Ranikhet Disease of PoultryDocument22 pagesRanikhet Disease of PoultryNadineNo ratings yet
- Herpes ZosterDocument6 pagesHerpes ZosterRonan suhendraNo ratings yet
- Medicine Lec.9 - Viral Infection IIDocument42 pagesMedicine Lec.9 - Viral Infection II7fefdfbea1No ratings yet
- ENTEROBACTERIACEAEDocument34 pagesENTEROBACTERIACEAEdrtsotlhe mogolegwaNo ratings yet
- Mumps NoteDocument4 pagesMumps Noteemmanuelnwa943No ratings yet
- How hormones like dopamine, serotonin, oxytocin and endorphins impact happinessDocument22 pagesHow hormones like dopamine, serotonin, oxytocin and endorphins impact happinessRabina PantaNo ratings yet
- Solid and Cystic Lesion of PancreasDocument27 pagesSolid and Cystic Lesion of PancreasRabina PantaNo ratings yet
- Caries ControlDocument19 pagesCaries ControlRabina PantaNo ratings yet
- Treatment of Maxillary SinusitisDocument15 pagesTreatment of Maxillary SinusitisRabina PantaNo ratings yet
- Asthma Diagnosis and TreatmentDocument16 pagesAsthma Diagnosis and TreatmentRabina PantaNo ratings yet
- End-of-Lifecare: Rabina Panta 1701938Document12 pagesEnd-of-Lifecare: Rabina Panta 1701938Rabina PantaNo ratings yet
- Solid and Cystic Lesion of PancreasDocument27 pagesSolid and Cystic Lesion of PancreasRabina PantaNo ratings yet
- DepressionDocument9 pagesDepressionRabina PantaNo ratings yet
- Understanding Autoimmune Hemolytic Anemia (AIHADocument28 pagesUnderstanding Autoimmune Hemolytic Anemia (AIHARabina PantaNo ratings yet
- Daleel EDocument44 pagesDaleel Ealiplus007No ratings yet
- Resume GROUP 9Document3 pagesResume GROUP 9Sicat Mark BantiyanNo ratings yet
- Improve Nursing Skills and Knowledge with Medical Case Studies and QuestionsDocument41 pagesImprove Nursing Skills and Knowledge with Medical Case Studies and Questionsjodymahmoud100% (1)
- Webrep - Cgi 4Document1 pageWebrep - Cgi 4viridiana bonillaNo ratings yet
- HS - I Don't Feel Weel TodayDocument10 pagesHS - I Don't Feel Weel Todaychie NbaNo ratings yet
- 2.standards of Midwifery PracticeDocument22 pages2.standards of Midwifery PracticeVeena DalmeidaNo ratings yet
- Potent Antioxidant Acacia catechu ExtractDocument1 pagePotent Antioxidant Acacia catechu ExtractmdibashaNo ratings yet
- Politics in Healing The Suppression and Manipulation of American Medicine (PDFDrive)Document501 pagesPolitics in Healing The Suppression and Manipulation of American Medicine (PDFDrive)Anonymous IjmLRYg69TNo ratings yet
- SMEDA Private HospitalDocument23 pagesSMEDA Private Hospitalomerzafar100% (1)
- Ams PHC Mop FinalDocument77 pagesAms PHC Mop FinalCNCMH LOONNo ratings yet
- COVID-19 poverty Philippines lockdowns job lossesDocument1 pageCOVID-19 poverty Philippines lockdowns job lossesRyza ParreñoNo ratings yet
- Bureau of Fire Protection First AidDocument7 pagesBureau of Fire Protection First AidRexelle RamosNo ratings yet
- IGC 2 - Element 7 - Chemical HazardsDocument67 pagesIGC 2 - Element 7 - Chemical HazardsHim SiwakotiNo ratings yet
- CBT Blissful MaterialDocument223 pagesCBT Blissful MaterialDanial Hassan80% (5)
- Who Pen 2020Document85 pagesWho Pen 2020Faye PalmaresNo ratings yet
- Last Week DataDocument15 pagesLast Week Datajaswant0% (1)
- Case StudyDocument44 pagesCase StudyPankaj AgrawalNo ratings yet
- Colostrum - How Does It Keep Health?Document9 pagesColostrum - How Does It Keep Health?JakirNo ratings yet
- Yamamoto Acupuncture PDFDocument17 pagesYamamoto Acupuncture PDFcarlos100% (1)
- The Journal of Contemporary Dental PracticeDocument7 pagesThe Journal of Contemporary Dental Practicegone goneNo ratings yet
- Basic Principles of Nursing EthicsDocument2 pagesBasic Principles of Nursing Ethicsalena volinaNo ratings yet
- Uputstvo Za OsiguranikaDocument1 pageUputstvo Za OsiguranikaSavkicZoranNo ratings yet
- AI en Medicina-NEJM 2023Document2 pagesAI en Medicina-NEJM 2023Walter ReyesNo ratings yet
- Tenses For OETDocument2 pagesTenses For OETGyby Nair100% (1)
- Add (Acute Diarrhoeal Disease)Document46 pagesAdd (Acute Diarrhoeal Disease)Mohamed Mahroof100% (1)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationLillabinNo ratings yet
- Case 4 Novartis Gilenya (Pain)Document19 pagesCase 4 Novartis Gilenya (Pain)phaynNo ratings yet
- Daftar Pustaka: Universitas Sumatera UtaraDocument5 pagesDaftar Pustaka: Universitas Sumatera UtaraNoona MuflihanaNo ratings yet
- 17 TYPES OF GOOD BACTERIA - The List of Most Beneficial Species of Probiotics Lactobacillus and Bifidobacteria - Ecosh LifeDocument30 pages17 TYPES OF GOOD BACTERIA - The List of Most Beneficial Species of Probiotics Lactobacillus and Bifidobacteria - Ecosh LifeCarl MacCordNo ratings yet
- Vietfair - Lịch triển lãm 2022 - EDocument3 pagesVietfair - Lịch triển lãm 2022 - EThao NguyenNo ratings yet