You might also like
- Day 3 - Common Session 2 - Ethical Issues in PC - DR PrabhaDocument70 pagesDay 3 - Common Session 2 - Ethical Issues in PC - DR Prabham debNo ratings yet
- Principles of Palliative Care 2nd PartDocument26 pagesPrinciples of Palliative Care 2nd PartDisala Ranaweera100% (1)
- Etics in The ICU - NewDocument9 pagesEtics in The ICU - NewGhinter MariusNo ratings yet
- Ethical Principles of Paternalism in NursingDocument10 pagesEthical Principles of Paternalism in NursingGladz C CadaguitNo ratings yet
- By Dr. Myra C. BritillerDocument72 pagesBy Dr. Myra C. BritillerCharleneBunquin100% (1)
- Ethical Challenges at The End of Life: Eyad Nashawati, MDDocument28 pagesEthical Challenges at The End of Life: Eyad Nashawati, MDRazaCreciaLastrillaMenesesNo ratings yet
- Nursing EthicsDocument8 pagesNursing EthicsJam AicaNo ratings yet
- Values of NursingDocument27 pagesValues of NursingJay-l Escuadra82% (22)
- Ethical Decision Making in Medical PracticeDocument12 pagesEthical Decision Making in Medical PracticeJamali GagahNo ratings yet
- Getting Whole, Getting Well: Healing Holistically from Chronic IllnessFrom EverandGetting Whole, Getting Well: Healing Holistically from Chronic IllnessRating: 5 out of 5 stars5/5 (1)
- Patient's Bill of Rights: Information For PatientsDocument5 pagesPatient's Bill of Rights: Information For PatientsMamemi AlonzoNo ratings yet
- Two Ethics Case ScenariosDocument3 pagesTwo Ethics Case ScenariosEguia NielNo ratings yet
- HPCA Chapter 3 v6Document14 pagesHPCA Chapter 3 v6saonone100% (1)
- Own Your Care: A Family Guide to Navigating Complex Illness, Changing Health, or Unexpected PrognosisFrom EverandOwn Your Care: A Family Guide to Navigating Complex Illness, Changing Health, or Unexpected PrognosisNo ratings yet
- Navigating Legal and Ethical Issues in Nursing and HealthcareDocument6 pagesNavigating Legal and Ethical Issues in Nursing and HealthcareAlyxen PelingenNo ratings yet
- Truth-telling and Withholding Information UW Department of Bioethics & HumanitiesDocument1 pageTruth-telling and Withholding Information UW Department of Bioethics & HumanitiesKarl Sean OctavianoNo ratings yet
- Legal and Ethical Issues in GeriatricsDocument5 pagesLegal and Ethical Issues in GeriatricsStephy Sojan100% (1)
- Week 3 PATIENTS RIGHTS AND RESPONSIBILITIES 19-20Document32 pagesWeek 3 PATIENTS RIGHTS AND RESPONSIBILITIES 19-20maha abdallahNo ratings yet
- Assignment-Legal and Ethical Issues in PicuDocument20 pagesAssignment-Legal and Ethical Issues in PicushahnazNo ratings yet
- Find Your Way: Illness, Doctors, and Healthcare. A Doctor's Guide to Taking Charge of Your Health and Navigating Modern Healthcare.From EverandFind Your Way: Illness, Doctors, and Healthcare. A Doctor's Guide to Taking Charge of Your Health and Navigating Modern Healthcare.No ratings yet
- 10 Things I Wish I’d Learned in Medical School: A Practical Guide to Sustainable HealthFrom Everand10 Things I Wish I’d Learned in Medical School: A Practical Guide to Sustainable HealthRating: 5 out of 5 stars5/5 (1)
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi100% (4)
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi0% (1)
- Fiel Angelo G. Mallari, RNDocument68 pagesFiel Angelo G. Mallari, RNfiel mallariNo ratings yet
- Becoming An Ethical PractitionerDocument5 pagesBecoming An Ethical Practitionerapi-702639694No ratings yet
- Ethical decision making for end-of-life careDocument19 pagesEthical decision making for end-of-life careErick MaulanaNo ratings yet
- Professionaladjustmentfornursingreviewer 101203232906 Phpapp02Document19 pagesProfessionaladjustmentfornursingreviewer 101203232906 Phpapp02Crystal Ann Monsale TadiamonNo ratings yet
- ElectiveDocument35 pagesElectivedeeNo ratings yet
- Pd5 Research PaperDocument8 pagesPd5 Research PaperpjcolitaNo ratings yet
- Physician Integrity: Why It Is InviolableDocument3 pagesPhysician Integrity: Why It Is InviolableAndrea Villagran100% (1)
- CODE OF ETHICSDocument10 pagesCODE OF ETHICSviswa chowdaryNo ratings yet
- BAPSDocument21 pagesBAPSayron600No ratings yet
- Beginning BioethicsDocument79 pagesBeginning BioethicsGilbert IskandarNo ratings yet
- Ethical Principles in Community Health NursingDocument24 pagesEthical Principles in Community Health Nursingjansanmathew33% (3)
- A Curious Woman's Guide to Urology: UTIs, Wet Pants, Stones, and More!From EverandA Curious Woman's Guide to Urology: UTIs, Wet Pants, Stones, and More!No ratings yet
- Legal and Ethical IssuesDocument22 pagesLegal and Ethical IssuesPratima Karki100% (1)
- Medical Ethics Principles for Patient CareDocument12 pagesMedical Ethics Principles for Patient CareMae Anne MahinayNo ratings yet
- ''Excuse Me Doctor! I've Got What?'': Taking Ownership of Your Health and Making Healthcare Reform Work for YouFrom Everand''Excuse Me Doctor! I've Got What?'': Taking Ownership of Your Health and Making Healthcare Reform Work for YouNo ratings yet
- GeroDocument7 pagesGeroJehanie LukmanNo ratings yet
- The Palliative Approach: A Resource for Healthcare WorkersFrom EverandThe Palliative Approach: A Resource for Healthcare WorkersRating: 4.5 out of 5 stars4.5/5 (3)
- Future Healthcare Today: How Technology is Revolutionizing Holistic WellnessFrom EverandFuture Healthcare Today: How Technology is Revolutionizing Holistic WellnessNo ratings yet
- Nomos Meaning "Custom" or "Law". This Reflects The Political Sense of The Word-A Group's RightDocument4 pagesNomos Meaning "Custom" or "Law". This Reflects The Political Sense of The Word-A Group's RightZoe Jisel LuzadasNo ratings yet
- We Were Better Together: Navigating Cancer as a Couple with Love, Practical Advice and Expert GuidanceFrom EverandWe Were Better Together: Navigating Cancer as a Couple with Love, Practical Advice and Expert GuidanceNo ratings yet
- Dr. Mohamed Mosaad Hasan MD, MPH, CPHQ, CPPS, GbssDocument48 pagesDr. Mohamed Mosaad Hasan MD, MPH, CPHQ, CPPS, GbssKristine Marie PateñoNo ratings yet
- Top Ethical Issues in NursingDocument6 pagesTop Ethical Issues in NursingKrizelle SanchezNo ratings yet
- The Underlying Principles of Ethical Patient CareDocument7 pagesThe Underlying Principles of Ethical Patient CareGulshanNo ratings yet
- Professionaladjustmentfornursingreviewer 101203232906 Phpapp02Document20 pagesProfessionaladjustmentfornursingreviewer 101203232906 Phpapp02Elaine Elhai LaineNo ratings yet
- Virtues of Health Care ProfessionalDocument24 pagesVirtues of Health Care ProfessionalMaritel Riego Ledesma100% (1)
- Sxetika Me Palliative CareDocument2 pagesSxetika Me Palliative CareKatrin DemertziNo ratings yet
- The 4 Box Method - Practical ApproachDocument39 pagesThe 4 Box Method - Practical ApproachramwshNo ratings yet
- Patients' Rights in HealthcareDocument45 pagesPatients' Rights in HealthcareCreciabullecerNo ratings yet
- K5-Ethical Aspect of Physician-Patient and Physician-Society RelationshipDocument29 pagesK5-Ethical Aspect of Physician-Patient and Physician-Society RelationshipJamali GagahNo ratings yet
- Informed Consent As An Ethical Issue in NursingDocument4 pagesInformed Consent As An Ethical Issue in NursingJIMOH Shamsudeen JideNo ratings yet
- Communication With and On Behalf of PatientsDocument133 pagesCommunication With and On Behalf of PatientsDes Anggraeni RuniasiwiNo ratings yet
- Doctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebDocument10 pagesDoctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebAdel AdlyNo ratings yet
- Lesson Plan Tot 609Document4 pagesLesson Plan Tot 609Bayu PermanaNo ratings yet
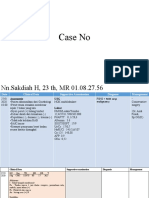
- Case NoDocument9 pagesCase NoBayu PermanaNo ratings yet
- Lesson Plan PR MentahDocument3 pagesLesson Plan PR MentahBayu PermanaNo ratings yet
- FirefightingDocument4 pagesFirefightingBayu PermanaNo ratings yet
- XCPT DEKIMANSUR 15-01-13 07.04.00Document5 pagesXCPT DEKIMANSUR 15-01-13 07.04.00Bayu PermanaNo ratings yet
- XCPT DEKIMANSUR 15-01-13 12.49.42Document5 pagesXCPT DEKIMANSUR 15-01-13 12.49.42Bayu PermanaNo ratings yet
- XCPT DEKIMANSUR 15-01-13 12.49.42Document5 pagesXCPT DEKIMANSUR 15-01-13 12.49.42Bayu PermanaNo ratings yet
- XCPT DEKIMANSUR 15-01-13 07.04.00Document5 pagesXCPT DEKIMANSUR 15-01-13 07.04.00Bayu PermanaNo ratings yet
- FDC TBDocument24 pagesFDC TBPanduRespatiNo ratings yet
- ManagementDocument66 pagesManagementBayu PermanaNo ratings yet
- Daftar Pustaka: Volume 1. New York: Plenum Publishing Corporation. 109-113Document2 pagesDaftar Pustaka: Volume 1. New York: Plenum Publishing Corporation. 109-113Bayu PermanaNo ratings yet
- Bayu Permana 030.09.045: Short Questions For Lecture in Community NutritionDocument3 pagesBayu Permana 030.09.045: Short Questions For Lecture in Community NutritionBayu PermanaNo ratings yet
- Project ManagementDocument14 pagesProject ManagementBayu PermanaNo ratings yet
- D Series: Instruction ManualDocument2 pagesD Series: Instruction ManualMartin del ValleNo ratings yet
- Philippine Legal CitationDocument72 pagesPhilippine Legal CitationArwella GregorioNo ratings yet
- Circuit Diagram Eng 5582-2-01Document95 pagesCircuit Diagram Eng 5582-2-01edolzaNo ratings yet
- UCT APM M2 U1 - TP Leadership QuestionnaireDocument4 pagesUCT APM M2 U1 - TP Leadership QuestionnaireLincolyn MoyoNo ratings yet
- Efficiently Transfer Stock Between PlantsDocument6 pagesEfficiently Transfer Stock Between PlantsSantosh KumarNo ratings yet
- Bee Unit-IiDocument98 pagesBee Unit-IiHemant Ingale100% (1)
- KiaOptima Seccion 002Document7 pagesKiaOptima Seccion 002Luis Enrique PeñaNo ratings yet
- Surface Wettability of Paper (Angle-of-Contact Method) : Standard Test Method ForDocument4 pagesSurface Wettability of Paper (Angle-of-Contact Method) : Standard Test Method ForfadjarNo ratings yet
- Brochure PILA Lamps and LuminairesDocument42 pagesBrochure PILA Lamps and Luminairesaldtol21No ratings yet
- Blood Smear PreparationDocument125 pagesBlood Smear PreparationKim RuizNo ratings yet
- The Effective of Geothermal Energy in BuDocument8 pagesThe Effective of Geothermal Energy in BuMeziane YkhlefNo ratings yet
- Foundation Fieldbus: Dataguard™ - Iec61158-2 - Isa/Sp50 - Type A - Extended TemperatureDocument1 pageFoundation Fieldbus: Dataguard™ - Iec61158-2 - Isa/Sp50 - Type A - Extended TemperatureJosé CallisayaNo ratings yet
- Adaboost With Totally Corrective Updates For Fast Face DetectionDocument6 pagesAdaboost With Totally Corrective Updates For Fast Face DetectionNguyen Quoc TrieuNo ratings yet
- Professional Industrial Engineering Program: Technical EnglishDocument15 pagesProfessional Industrial Engineering Program: Technical EnglishFabio fernandezNo ratings yet
- CSA09 Programming in Java MediumDocument25 pagesCSA09 Programming in Java Mediumsometimesop7934No ratings yet
- Impact of Microfinance On Women's Empowerment: A Case Study On Two Microfinance Institutions in Sri LankaDocument11 pagesImpact of Microfinance On Women's Empowerment: A Case Study On Two Microfinance Institutions in Sri Lankamandala jyoshnaNo ratings yet
- Data Table CarbonDocument2 pagesData Table Carbonyodaswarrior33% (15)
- SC Project Closeout Report v6Document27 pagesSC Project Closeout Report v6SateeshIngoleNo ratings yet
- ERA News Mar 23 - Final - 0Document10 pagesERA News Mar 23 - Final - 0Băltoiu Son AlisaNo ratings yet
- Prelims Module On Forensic 1Document17 pagesPrelims Module On Forensic 1Vanessa CorpuzNo ratings yet
- FINAL Please Be Informed That Your Termination From Office Is Not Intended To Be PersonalDocument9 pagesFINAL Please Be Informed That Your Termination From Office Is Not Intended To Be PersonalShareff ChamplainNo ratings yet
- Squidpy: A Scalable Framework For Spatial Omics Analysis: ArticlesDocument14 pagesSquidpy: A Scalable Framework For Spatial Omics Analysis: ArticlesXin XuNo ratings yet
- June 28th Altran Capital Market Day Presentation DeckDocument52 pagesJune 28th Altran Capital Market Day Presentation Deckvenkata.krishnan100% (1)
- Akhtamov A.A. - Destination C1-C2, Test CollectionDocument37 pagesAkhtamov A.A. - Destination C1-C2, Test CollectionNguyen NhiNo ratings yet
- 11.1 Exam Practice 30 U11Document6 pages11.1 Exam Practice 30 U11Đỗ LoanNo ratings yet
- SchoolopeningdocxDocument1 pageSchoolopeningdocxElena BarsukovaNo ratings yet
- DNV OS-B101 Metallic MaterialsDocument48 pagesDNV OS-B101 Metallic MaterialsBoni Luck100% (1)
- Dyno InstructionsDocument2 pagesDyno InstructionsAlicia CarrNo ratings yet
- 4.2 Force and Motion 1Document19 pages4.2 Force and Motion 1ammarsyahmiNo ratings yet
- Overview of Common Communication Challenges and TipsDocument7 pagesOverview of Common Communication Challenges and TipsTinyEYE Therapy ServicesNo ratings yet